


 超级微创手术:胃肠内镜
超级微创手术:胃肠内镜



Preface: Embracing a New Era of “Super Minimally Invasive Surgery”

Preface: Pioneering the SMIS Philosophy
Super Minimally Invasive Surgery: An Inevitable Choice for Humanity
Part One General Introduction to Super Minimally Invasive Surgery
Chapter 1 The Birth and Significance of Super Minimally Invasive Theory
1.1 The Rapid Development of Gastrointestinal Surgery, the Emergence of the Super Minimally Invasive Theory
1.2 Super Minimally Invasive Theory Has Profound Guiding Significance for Future Surgical Therapeutics
1.3 Guided by the Super Minimally Invasive Theory, Super Minimally Invasive Surgery is Booming

References
Chapter 2 The Super Minimally Invasive Theoretical System
2.1 The Definition and Implementation Principles of Super Minimally Invasive Surgery
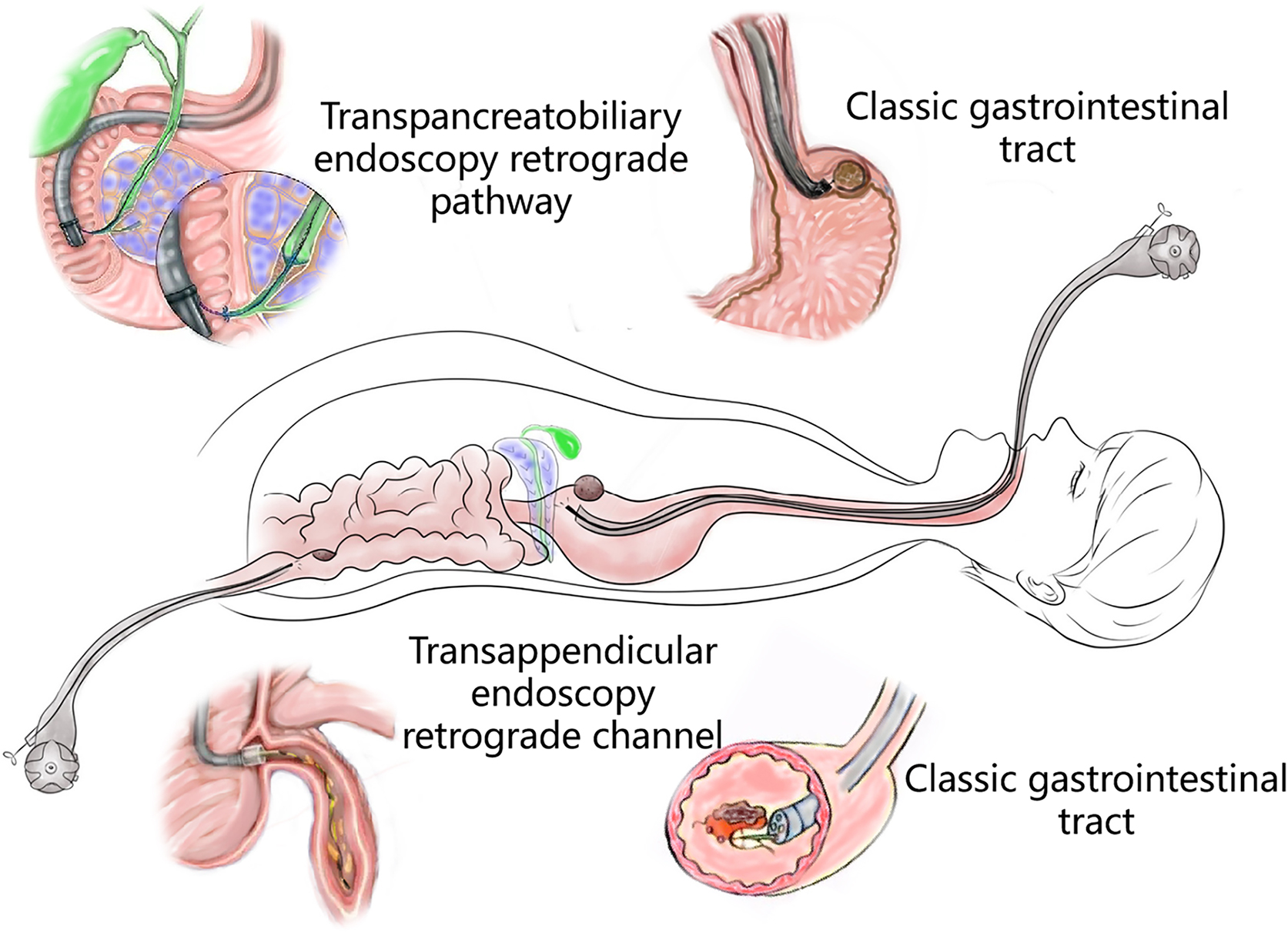
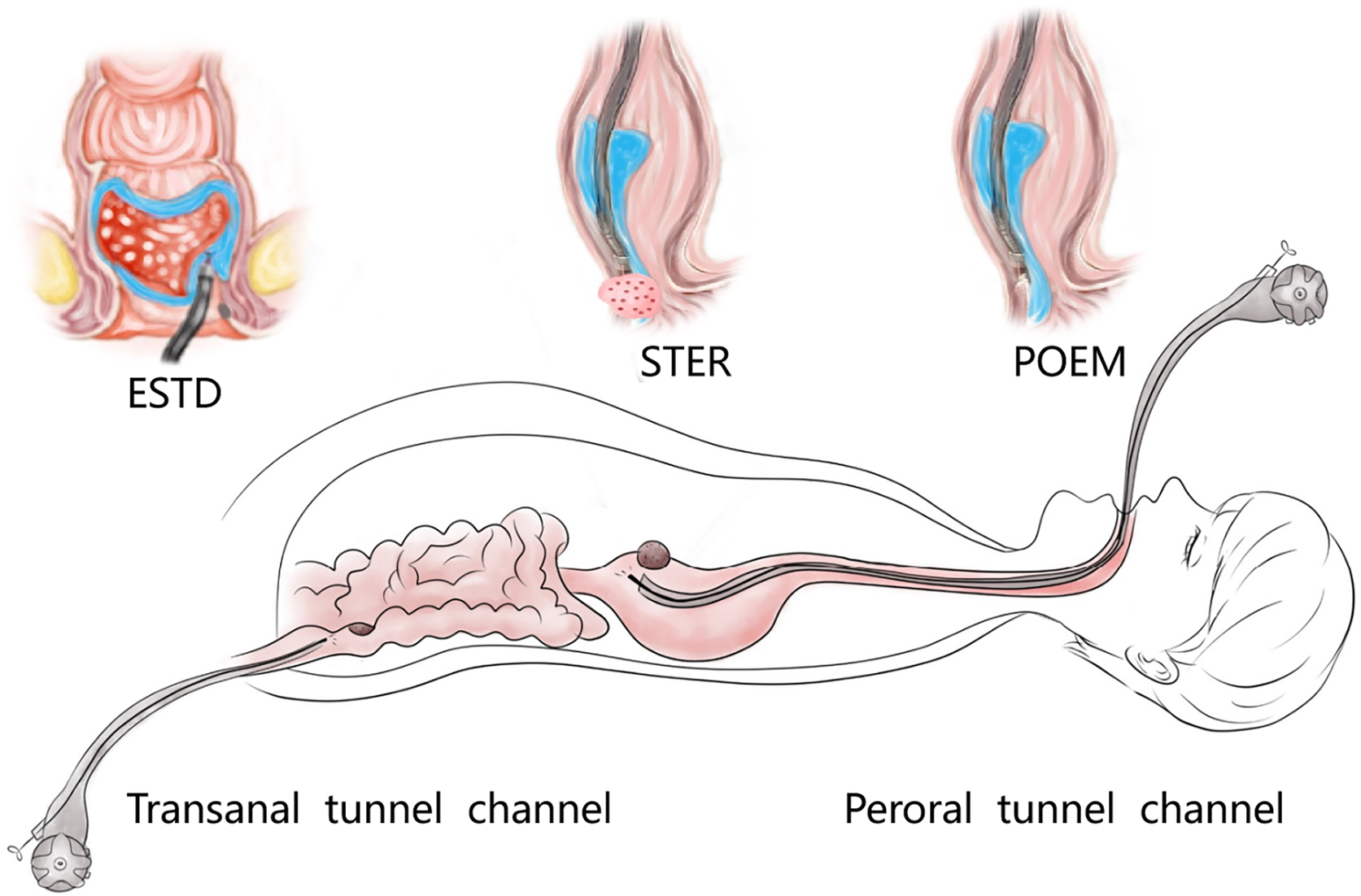
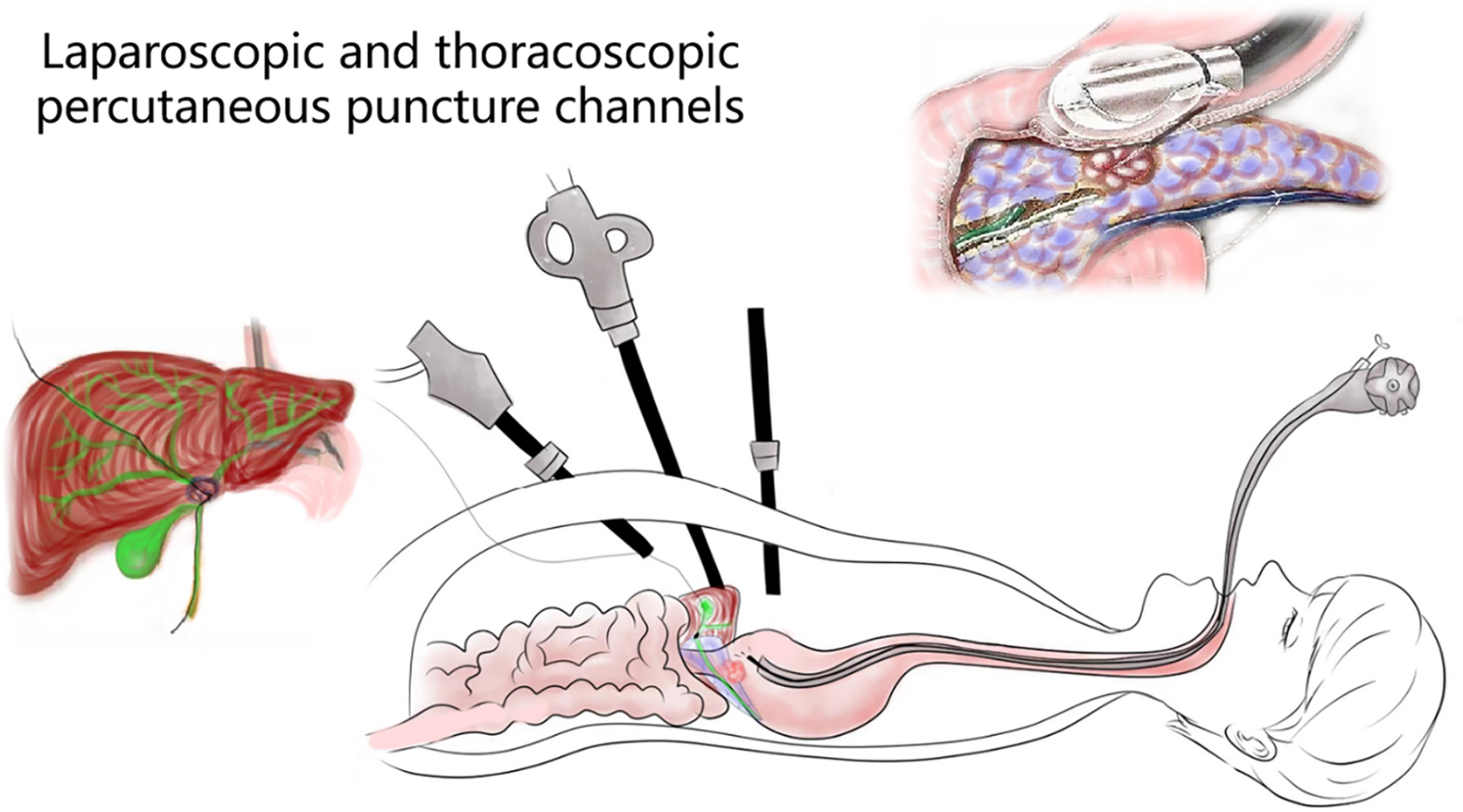
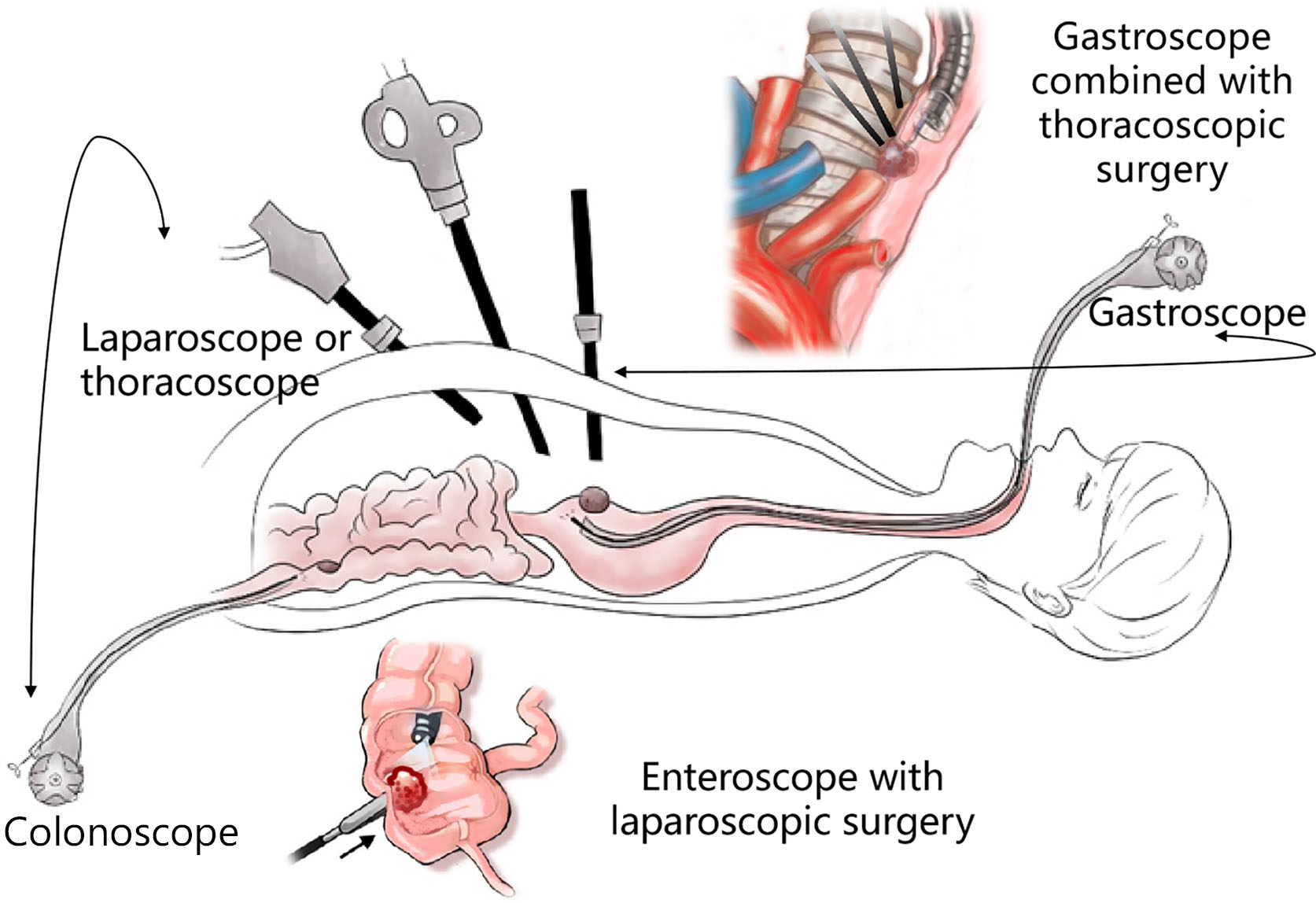
2.2 The Four Channels of Super Minimally Invasive Surgery
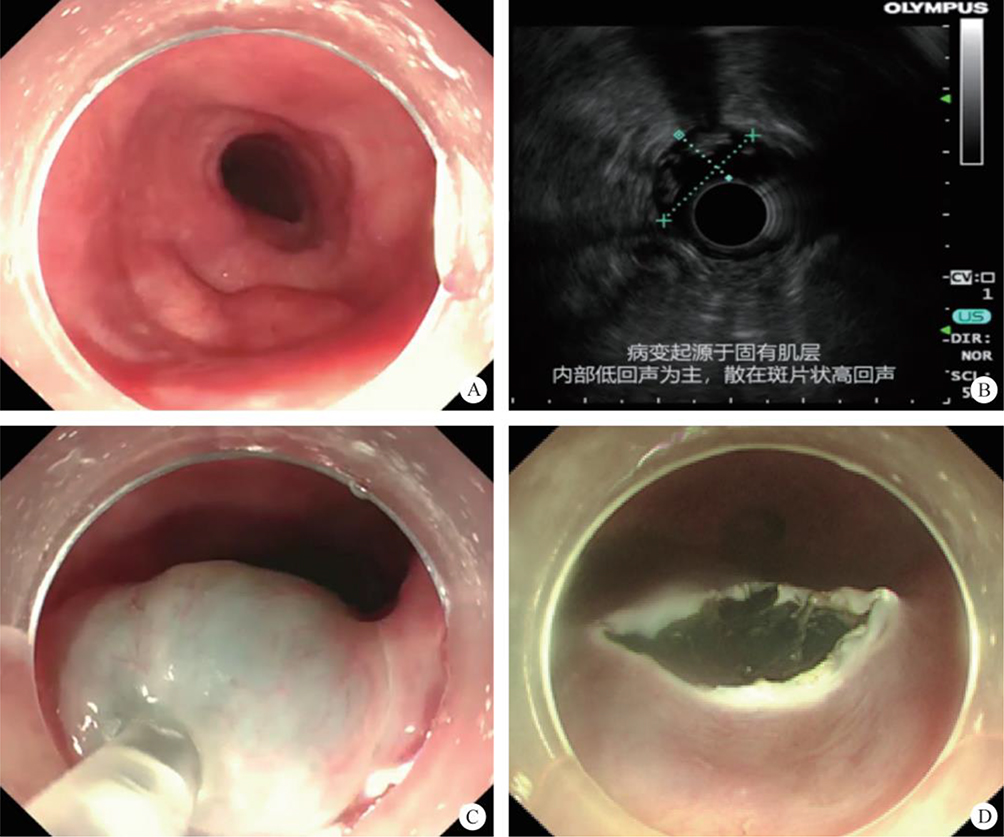
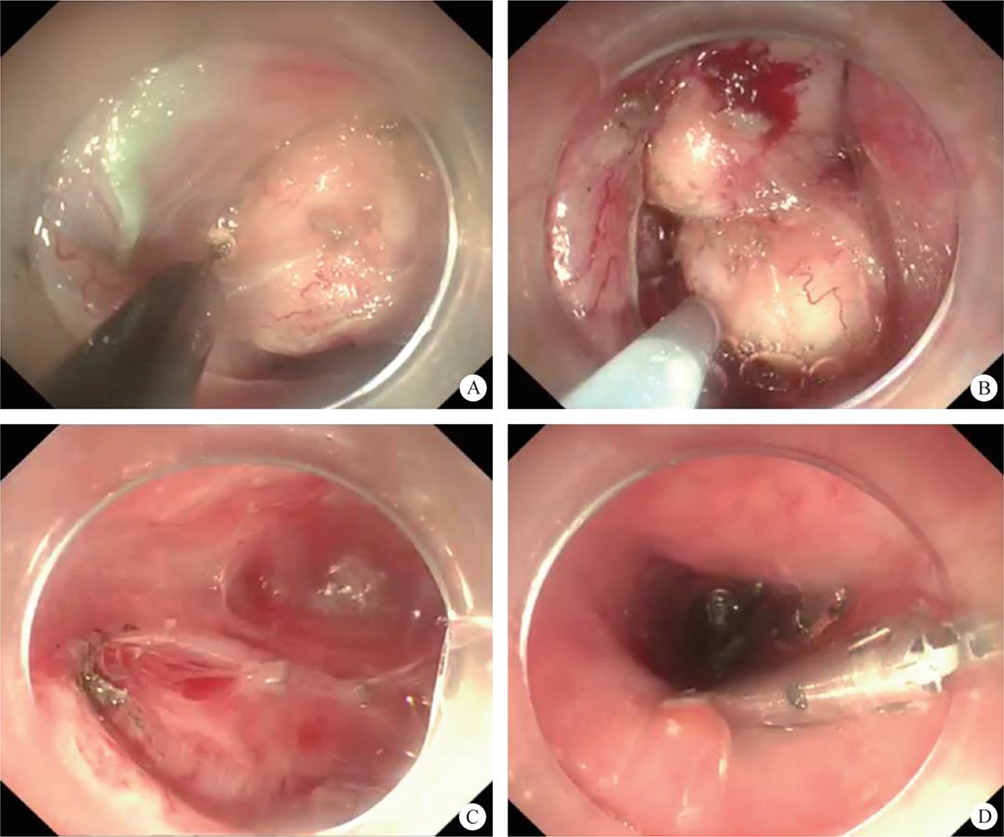
(1) A modified endoscopic resection of the entire thickness of a gastrointestinal stroma tumor: A new sealing technique based on the principles of super minimally invasive surgery (video 2.1 (See online resources)).
(2) Novel endoscopic papillectomy technique for reducing postoperative adverse events (video 2.2 (See online resources)).
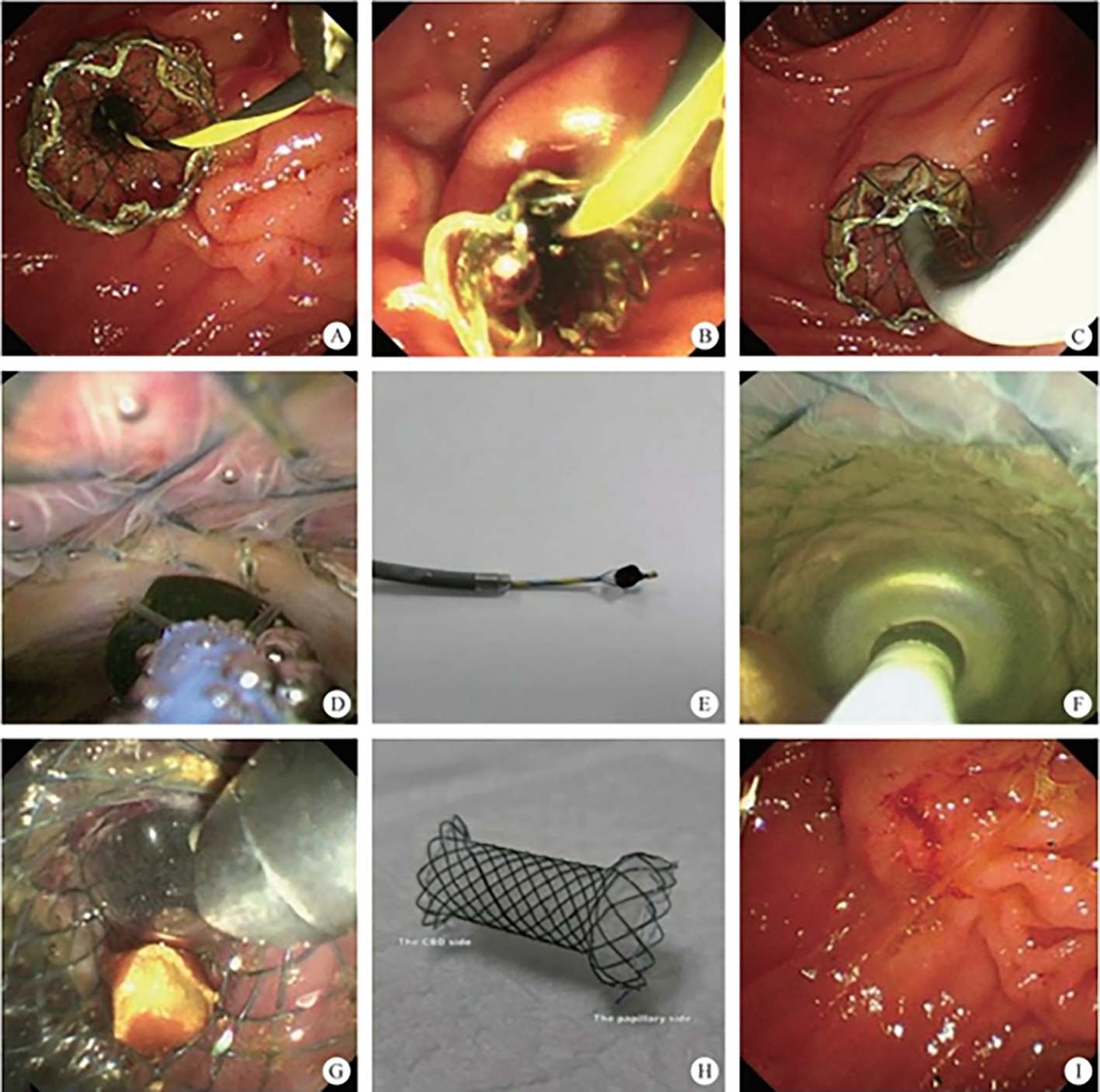
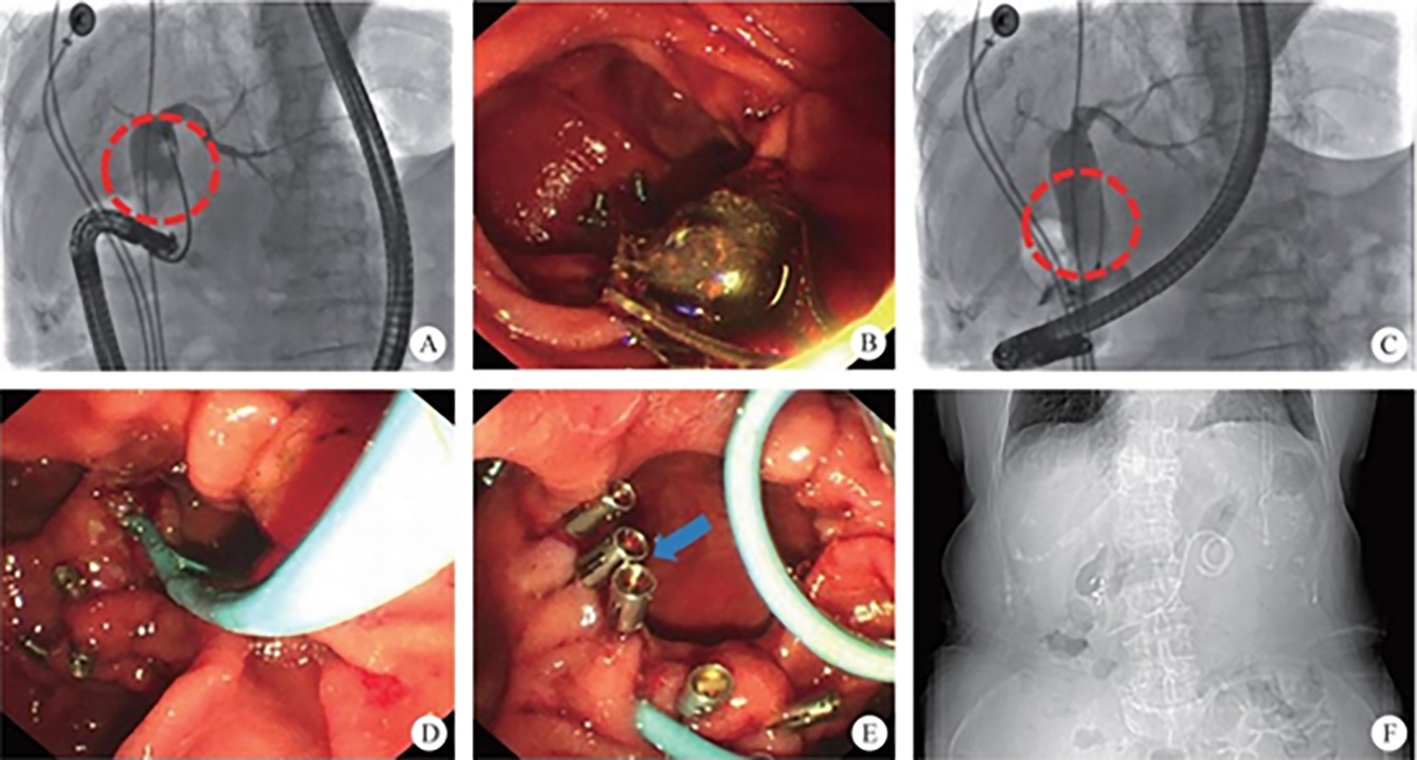
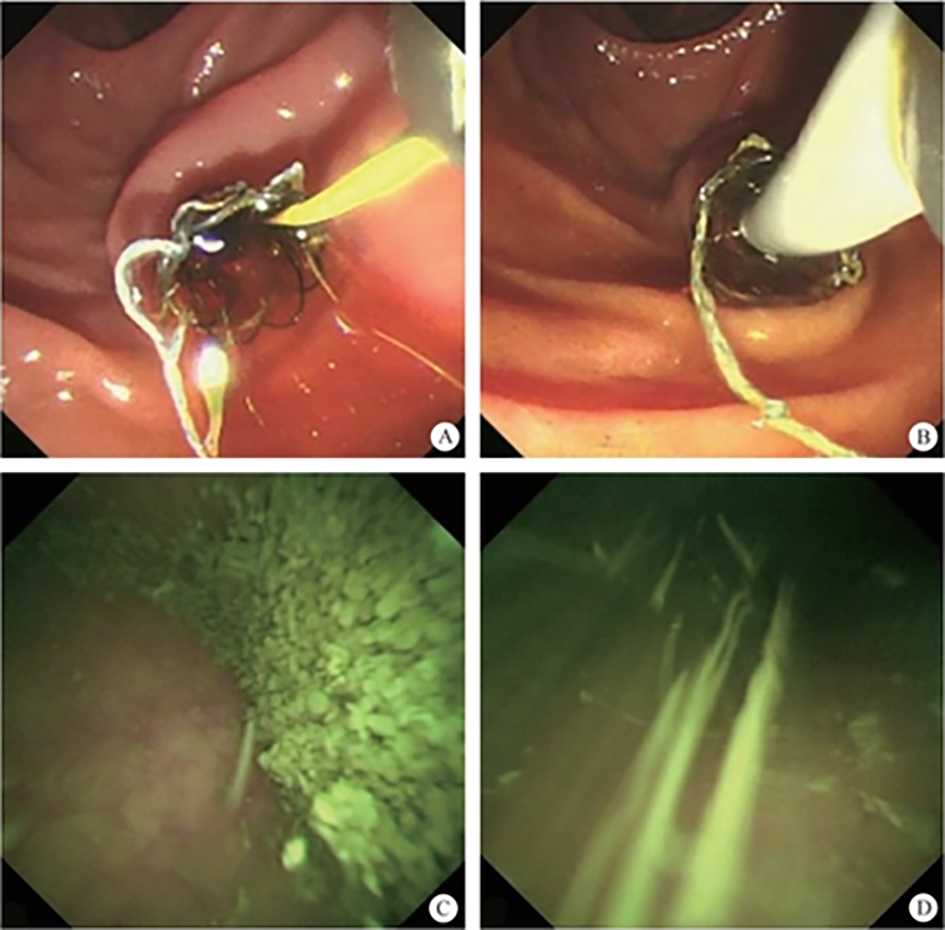
(3) Successful endoscopic transgastric retrieval of a plastic stent that migrated into the abdominal cavity during pancreatic fistula drainage (video 2.3 (See online resources)).
(4) Endoscopic retrieval of a migrated lumen-apposing metal stent into the abdominal cavity during transluminal drainage (video 2.4 (See online resources)).
(5) Incidental discovery of a pancreatic ductal adenocarcinoma during percutaneous cholangioscopy through a T-tube tract (video 2.5 (See online resources)).
(6) Three pancreatic duct lesions discovered at an early stage in a patient by cholangioscopy (video 2.6 (See online resources)).
(1) Autologous skin-grafting surgery for the prevention of esophageal stenosis after complete circular endoscopic submucosal tunnel dissection (video 2.7 (See online resources)).
(2) Challenging use of the digestive endoscopic tunnel technique to treat schwannoma originating in the trachea (video 2.8 (See online resources)).
(3) Endoscopic submucosal tunnel dissection with an elastic traction device for a circumferential superficial esophageal neoplasm (video 2.9 (See online resources)).
(4) Magnetic multi-directional anchoring-guided endoscopic submucosal tunnel dissection for large gastric lesions (video 2.10 (See online resources)).
(5) Simultaneous performance of one-tunnel per-oral endoscopic myotomy, submucosal tunnel endoscopic resection, and peroral diverticulotomy (video 2.11 (See online resources)).
(6) Peroral endoscopic myotomy with simultaneous submucosal and muscle dissection for achalasia with severe interlayer adhesions (video 2.12 (See online resources)).
(7) Moving the knife’s tip on the thoracic aorta: high-risk submucosal tunneling endoscopic resection procedure for a puzzling submucosal tumor in the esophagus ((video 2.13 (See online resources)).
(8) Prepyloric submucosal tunneling endoscopic resection for a case of inflammatory mass (video 2.14 (See online resources)).
(III) Approach via the puncture channel
(1) Rendezvous-assisted endoscopic retrograde pancreatography in a patient with annular pancreas and coexisting pancreas divisum (video 2.15 (See online resources)).
(2) Novel treatment of pancreatic cystic neoplasms: EUS-guided radiofrequency ablation combined with lauromacrogol ablation (video 2.16 (See online resources)).
(3) Spyglass discovery of a mucinous cystic neoplasm by introducing an optical fiber into the cyst through a 19G needle during EUS examination (video 2.17 (See online resources)).
3. Video of a classic case. Flexible choledochoscopy via the cystic duct combined with laparoscopic cholecystectomy for the treatment of cholelithiasis (video 2.18 (See online resources)).
2.3 The Techniques of Super Minimally Invasive Surgery


References
Chapter 3 Nomenclature in Super Minimally Invasive Surgery and Surgical Record Rules
3.1 Rules of Surgical Nomenclature
| No. | Name | Abbreviation |
| 1 | Peroral super minimally invasive surgery by non-full-thickness resection of a superior esophageal papilloma | Peroral SMIS-non FTR for SEP |
| 2 | Peroral super minimally invasive surgery by non-full-thickness resection of a middle esophageal high-grade intraepithelial neoplasm | Peroral SMIS-non FTR for MEHIN |
| 3 | Peroral super minimally invasive surgery by non-full-thickness resection of an inferior esophageal squamous cell carcinoma | Peroral SMIS-non FTR for IESCC |
| 4 | Peroral super minimally invasive surgery by non-full-thickness resection of a middle esophageal granular cell tumor | Peroral SMIS-non FTR for MEGCT |
| 5 | Peroral super minimally invasive surgery by full-thickness resection of an early adenocarcinoma on the gastroesophageal junction | Peroral SMIS–FTR for EAC on GEJ |
| 6 | Peroral super minimally invasive surgery by full-thickness resection of an inferior esophageal leiomyoma | Peroral SMIS–FTR for IEL |
| 7 | Per-tunnel super minimally invasive surgery by non-full-thickness resection of a middle esophageal carcinoma | Per-tunnel SMIS-non FTR for MEC |
| 8 | Per-tunnel super minimally invasive resection of an inferior esophageal leiomyoma | Per-tunnel SMIR for IEL |
| 9 | Per-tunnel super minimally invasive resection of a gastric stromal tumor on the gastroesophageal junction | Per-tunnel SMIR for GST on GEJ |
| 10 | Per-multi-cavity super minimally invasive resection of a middle esophageal leiomyoma | Per-multi-cavity SMIR for MEL |
| No. | Name | Abbreviation |
| 1 | Peroral super minimally invasive surgery by non-full-thickness resection for gastric high-grade intraepithelial neoplasia on the greater curvature of the gastric body | Peroral SMIS-non FTR for GHIN on the greater curvature of the gastric body |
| 2 | Peroral super minimally invasive surgery by non-full-thickness resection of a gastric carcinoma on the anterior wall of the gastric antrum | Peroral SMIS-non FTR for GC on the anterior wall of the gastric antrum |
| 3 | Peroral super minimally invasive surgery by non-full-thickness resection of a gastric leiomyoma on the lesser curvature of the gastric body | Peroral SMIS-non FTR for GL on the lesser curvature of the gastric body |
| 4 | Peroral super minimally invasive surgery by non-full-thickness resection of a gastric neuroendocrine tumor on the posterior wall of the gastric antrum | Peroral SMIS-non FTR for GNET on the posterior wall of the gastric antrum |
| 5 | Peroral super minimally invasive surgery by non-full-thickness resection of a gastric lipoma on the posterior wall of the gastric body | Peroral SMIS-non FTR for GL on the posterior wall of the gastric body |
| 6 | Peroral super minimally invasive surgery by full-thickness resection of a gastric glomus tumor on the gastric angle | Peroral SMIS–FTR for GGT on the gastric angle |
| 7 | Peroral super minimally invasive surgery by full-thickness resection of a gastric carcinoma on the greater curvature of the gastric body | Peroral SMIS–FTR for GC on the greater curvature of the gastric body |
| 8 | Peroral super minimally invasive surgery by full-thickness resection of a gastric stromal tumor on the greater curvature of gastric fundus | Peroral SMIS–FTR for GST on the greater curvature of the gastric fundus |
| 9 | Per-tunnel super minimally invasive surgery by non-full-thickness resection of a gastric carcinoma on the greater curvature of the gastric antrum | Per-tunnel SMIS-non FTR for GC on the greater curvature of the gastric antrum |
| 10 | Per-multi-cavity super minimally invasive resection of a gastric carcinoma on the anterior wall of the gastric body | Per-multi-cavity SMIR for GC on the anterior wall of the gastric body |
| 11 | Per-multi-cavity super minimally invasive resection of a gastric stromal tumor on the gastric angle | Per-multi-cavity SMIR for GST on the gastric angle |
| No. | Name | Abbreviation |
| 1 | Peroral super minimally invasive surgery by non-full-thickness resection of a duodenal bulb neuroendocrine tumor | Peroral SMIS-non FTR for DBNET |
| 2 | Peroral super minimally invasive surgery by non-full-thickness resection of a duodenal adenoma on the duodenal descending part | Peroral SMIS-non FTR for DA on the duodenal descending part |
| 3 | Peroral super minimally invasive surgery by non-full-thickness resection of a duodenal carcinoma on the duodenal descending part | Peroral SMIS-non FTR for DC on the duodenal descending part |
| 4 | Peroral super minimally invasive surgery by full-thickness resection of a duodenal bulb leiomyoma | Peroral SMIS–FTR for DBL |
| 5 | Peroral super minimally invasive resection of a duodenal papillary adenoma | Peroral SMIR for DPA |
| 6 | Peroral super minimally invasive resection of an early duodenal papillary carcinoma | Peroral SMIR for EDPC |
| 7 | Per-tunnel super minimally invasive resection of a duodenal bulb stromal tumor | Per-tunnel SMIR for DBST |
| 8 | Per-multi-cavity super minimally invasive resection of a duodenal carcinoma on the duodenal descending part | Per-multi-cavity SMIR for DC on the duodenal descending part |
| 9 | Peroral super minimally invasive surgery by non-full-thickness resection of a jejunum adenoma | Peroral SMIS-non FTR for JA |
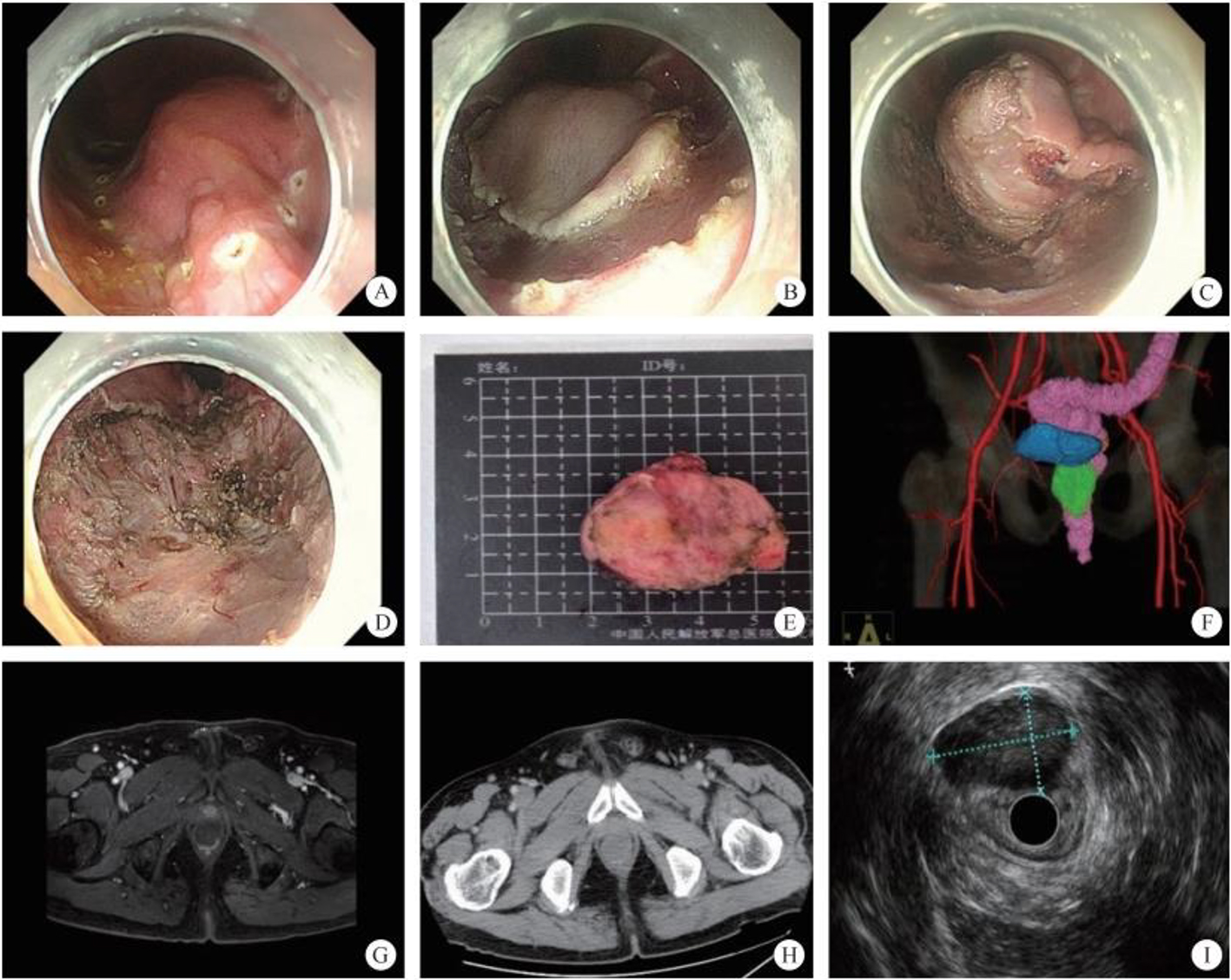
| 10 | Transanal super minimally invasive resection of an ileal stromal tumor | Transanal SMIR for IST |
| No. | Name | Abbreviation |
| 1 | Transanal super minimally invasive surgery by non-full-thickness resection of a sigmoid colon adenoma | Transanal SMIS-non FTR for SCA |
| 2 | Transanal super minimally invasive surgery by non-full-thickness resection of a descending colon lipoma | Transanal SMIS-non FTR for DCL |
| 3 | Transanal super minimally invasive surgery by full-thickness resection for an ascending colon adenocarcinoma | Transanal SMIS-non FTR for ACAC |
| 4 | Per-tunnel super minimally invasive surgery by non-full-thickness resection of a rectal adenocarcinoma | Per-tunnel SMIS-non FTR for RAC |
| 5 | Per-multi-cavity super minimally invasive resection of a neuroendocrine tumor of the appendix | Per-multi-cavity SMIR for ANET |
| 6 | Per-multi-cavity super minimally invasive resection of a cecal stromal tumor | Per-multi-cavity SMIR for CST |
| No. | Name | Abbreviation |
| 1 | Peroral super minimally invasive incision for middle esophageal cyst | Peroral SMII for MEC |
| 2 | Peroral super minimally invasive incision for superior esophageal diverticulum | Peroral SMII for SED |
| 3 | Peroral super minimally invasive incision for inferior benign esophageal stenosis | Peroral SMII for IBES |
| 4 | Peroral super minimally invasive E myotomy for achalasia | Peroral SMIM for achalasia |
| 5 | Peroral super minimally invasive myotomy for diffuse esophageal spasm | Peroral SMIM for DES |
| 6 | Peroral super minimally invasive myotomy for hypertrophic pyloric | Peroral SMIM for HP |
| 7 | Transanal super minimally invasive incision for benign jejunum stenosis | Transanal SMII for BJS |
| 8 | Transanal super minimally invasive incision for benign rectal stenosis | Transanal SMII for BRS |
| No. | Name | Abbreviation |
| 1 | Per-cutaneous-puncture ultrasound-guided super minimally invasive biliary drainage for primary sclerosing cholangitis | Per-cutaneous-puncture US-guided SMIBD for PSC |
| 2 | Per-gastric-puncture endoscopic ultrasound-guided super minimally invasive biliary drainage for acute suppurative cholecystitis | Per-gastric-puncture EUS-guided SMIBD for ASC |
| 3 | Per-duodenal-papilla super minimally invasive biliary drainage for acute suppurative cholangitis | Per-duodenal-papilla SMIBD for ASC |
| 4 | Per-duodenal-papilla super minimally invasive biliary drainage for choledochoduodenal fistula | Per-duodenal-papilla SMIBD for CF |
| 5 | Peroral super minimally invasive biliary drainage for biliary perforation | Peroral SMIBD for BP |
| 6 | Peroral super minimally invasive drainage for choledochoduodenal fistula | Peroral SMID for CF |
| 7 | Per-duodenal-papilla super minimally invasive drainage for biliary stenosis | Per-duodenal-papilla SMID for BS |
| 8 | Per-duodenal-papilla super minimally invasive pancreatic duct drainage for incomplete pancreas divisum | Per-duodenal-papilla SMIPD for incomplete PD |
| 9 | Per-duodenal-papilla super minimally invasive pancreatic drainage for complete pancreas divisum | Per-duodenal-papilla SMIPD for complete PD |
| 10 | Per-gastric-puncture endoscopic ultrasound-guided super minimally invasive drainage for pancreatic pseudocyst | Per-gastric-puncture EUS-guided SMID for PPC |
| 11 | Per-gastric-puncture endoscopic ultrasound-guided super minimally invasive drainage for pancreatic walled-off necrosis | Per-gastric-puncture EUS-guided SMID for PWN |
| 12 | Peroral super minimally invasive pancreatic drainage for chronic pancreatitis | Peroral SMIPD for CP |
| 13 | Peroral super minimally invasive pancreatic drainage for pancreatic fistula | Peroral SMIPD for PF |
| 14 | Per-duodenal-papilla super minimally invasive pancreatic drainage for pancreatic stenosis | Per-duodenal-papilla SMIPD for PS |
| 15 | Per-duodenal-papilla super minimally invasive pancreatic drainage for disconnected pancreatic syndrome | Per-duodenal-papilla SMIPD for DPS |
| No. | Name | Abbreviation |
| 1 | Per-duodenal-papilla super minimally invasive extract for cholecystolithiasis | Per-duodenal-papilla SMIE for cholecystolithiasis |
| 2 | Peroral endoscopic ultrasound-guided super minimally invasive extract for cholecystolithiasis | Peroral EUS-guided SMIE for cholecystolithiasis |
| 3 | Per-duodenal-papilla super minimally invasive extract under cholangioscopy for biliary stone | Per-duodenal-papilla SMIE under cholangioscopy for BS |
| 4 | Peroral super minimally invasive extract for biliary stone after liver transplantation | Peroral SMIE for BS after LT |
| 5 | Peroral super minimally invasive extract for extrahepatic biliary stone | Peroral SMIE for EBS |
| 6 | Per-duodenal-papilla super minimally invasive extract for biliary pancreatitis | Per-duodenal-papilla SMIE for BP |
| 7 | Peroral super minimally invasive extract for pancreatic stone | Peroral SMIE for PS |
| No. | Name | Abbreviation |
| 1 | Peroral super minimally invasive anti-reflux surgery for gastroesophageal reflux disease | Peroral SMIARS for GERD |
| 2 | Peroral super minimally invasive radiofrequency ablation for gastroesophageal reflux disease | Peroral SMIRA for GERD |
| 3 | Peroral super minimally invasive ablation for middle esophageal cyst | Peroral SMIA for MEC |
| 4 | Peroral super minimally invasive radiofrequency ablation for superior esophageal low-grade intraepithelial neoplasia | Peroral SMIRA for SELIN |
| 5 | Peroral super minimally invasive radiofrequency ablation for low-grade intraepithelial neoplasia on the anterior wall of the gastric antrum | Peroral SMIRA for GLIN on the Anterior Wall of the gastric antrum |
| 6 | Peroral super minimally invasive ablation for gastric antral telangiectasia | Peroral SMIA for GAT |
| 7 | Per-gastric-puncture endoscopic ultrasound-guided super minimally invasive ablation for pancreatic cystic neoplasm | Per-gastric-puncture EUS-guided SMIA for PCN |
| 8 | Peroral super minimally invasive closure for esophagomediastinal fistula | Peroral SMIC for EMF |
| 9 | Peroral super minimally invasive closure for esophagotracheal fistula | Peroral SMIC for ETF |
3.2 Recording Rules for Super Minimally Invasive Surgery
3.2.1 SMIS Excision Methods and the Nomenclature of Endoscopic Techniques
3.2.2 Examples of SMIS Surgical Records
3.3 Surgical Items and Diseases
| Disease | SMIS Item | Definition |
| Biliary stone | Peroral super minimally invasive extraction | Peroral endoscopic removal of extrahepatic bile duct stone while preserving the function of the papillary sphincter, including basket extraction under direct vision, balloon extraction under direct vision, extraction by attraction under direct vision |
| Gallbladder stone | Peroral super minimally invasive extraction | Peroral endoscopic removal of gallbladder stones |
| Acute suppurative cholangitis | Peroral super minimally invasive drainage | Peroral endoscopic drainage of acute suppurative cholangitis |
| Gastric stromal tumor | Peroral super minimally invasive resection | Peroral endoscopic total resection of local gastric stromal tumors |
| Early gastric cancer | Peroral super minimally invasive resection | Peroral endoscopic total resection of local early gastric cancer |
| Early esophageal cancer | Peroral super minimally invasive resection | The technique of peroral endoscopic total resection locally of early esophageal cancer |
| Duodenal papillary adenoma | Peroral super minimally invasive resection | Peroral endoscopic total resection of a local duodenal papillary adenoma |
| Early colorectal cancer | Transanal super minimally invasive resection | Transanal endoscopic total resection of local early colorectal cancer |
| Gastroesophageal reflux disease | Peroral super minimally invasive anti-reflux | Peroral endoscopic treatment of gastroesophageal reflux |
| Barrett esophagus | Peroral super minimally invasive resection | Peroral endoscopic total resection of local esophageal lesions |
| Esophagomediastinal fistula | Peroral super minimally invasive closure for esophagomediastinal fistula | Peroral endoscopic closure of esophagome diastinal fistula |
| Appendicitis | Transanal super minimally invasive surgery | Transanal endoscopic removal of appendicular lithiasis |
| Benign esophageal stricture | Peroral super minimally invasive incision | Peroral endoscopic incision of the benign stricture segment to treat swallowing difficulties |
| Biliary stenosis, biliary fistula | Per-nasal super minimally invasive drainage | Used to place the nasobiliary drainage tube nasally; it thus plays the role of a drain |
| Gallbladder polyp | Peroral super minimally invasive resection | Peroral endoscopic resection of gallbladder polyps |
| Disease | SMIS Item | Definition |
| Early esophageal cancer | Per-tunnel super minimally invasive resection | Per-tunnel endoscopic resection of early esophageal cancer |
| Early gastric cancer | Per-tunnel super minimally invasive resection | Per-tunnel endoscopic resection of early gastric cancer |
| Early colorectal cancer | Per-tunnel super minimally invasive resection | Per-tunnel endoscopic resection of early colorectal cancer |
| Esophageal stromal tumor | Per-tunnel super minimally invasive resection | Per-tunnel endoscopic resection of esophageal stromal tumors |
| Submucosal mass at the esophagogastric junction | Per-tunnel super minimally invasive resection | Per-tunnel endoscopic resection of the submucosal mass at the esophagogastric junction |
| Small intestinal submucosal mass | Per-tunnel super minimally invasive resection | Per-tunnel endoscopic resection of the submucosal mass of the small intestine |
| Prepyloric submucosal mass | Per-tunnel super minimally invasive resection | Per-tunnel endoscopic resection of the prepyloric submucosal mass |
| Achalasia | Per-tunnel super minimally invasive incision | Per-tunnel endoscopic myotomy of the lower esophageal sphincter to treat achalasia, so as to relieve swallowing difficulties |
| Gastroparesis | Per-tunnel super minimally invasive incision | Per-tunnel endoscopic myotomy of the pyloric sphincter to treat gastroparesis |
| Esophageal diverticulum | Per-tunnel super minimally invasive incision | Per-tunnel penetration of the submucosal layer of the lower edge of the esophageal diverticulum and incision of the muscle layer of the ridge, so as to cure the disease |
| Disease | SMIS Item | Definition |
| Encapsulated effusion | Per-puncture channel super minimally invasive drainage | Encapsulated effusion aimed at preserving the integrity of the original tissue and the anatomical structure of the organ while achieving the objective of curing a disease |
| Pancreatic pseudocyst | Per-puncture channel super minimally invasive drainage | Endoscopic ultrasound-guided insertion of a puncture needle into the pseudocyst, fitting of a drainage stent in the cyst using a guide wire, to perform a gastrostomy or a cystoduodenostomy, to drain the internal cystic fluid of the pseudocyst |
| Biliary obstruction | Per-puncture channel super minimally invasive drainage | Endoscopic ultrasound-guided puncture of the dilated intra-and extrahepatic bile duct, to establish a channel between the bile duct and the digestive tract with the aid of a stent, to resolve biliary obstruction |
| Pancreatic cystic tumor | Per-puncture channel super minimally invasive ablation | Endoscopic ultrasound-guided entry into the pancreatic cystic tumor by puncturing the wall of the digestive tract to carry out chemical or physical ablation therapies |
| Gallbladder stone | Per-puncture channel super minimally invasive extraction | Endoscopic ultrasound-guided entry into the gallbladder to perform stone extraction |
| Encapsulated necrosis | Per-puncture channel super minimally invasive extraction | Endoscopic ultrasound-guided penetration of the gastric wall or the duodenal wall to enter the necrotic area, to establish a channel between the necrotic area and the wall of the digestive tract, dilatation using a balloon dilator to allow the endoscope to enter, and removal of the necrotic tissues by applying several tools such as a basket, foreign body forceps, a snare, etc. |
| Mediastinal, abdominal, pelvic abscess | Per-puncture channel super minimally invasive drainage | Endoscopic ultrasound-guided entry into the abscess site by puncturing the wall of the digestive tract for drainage |
| Disease | SMIS Item | Definition |
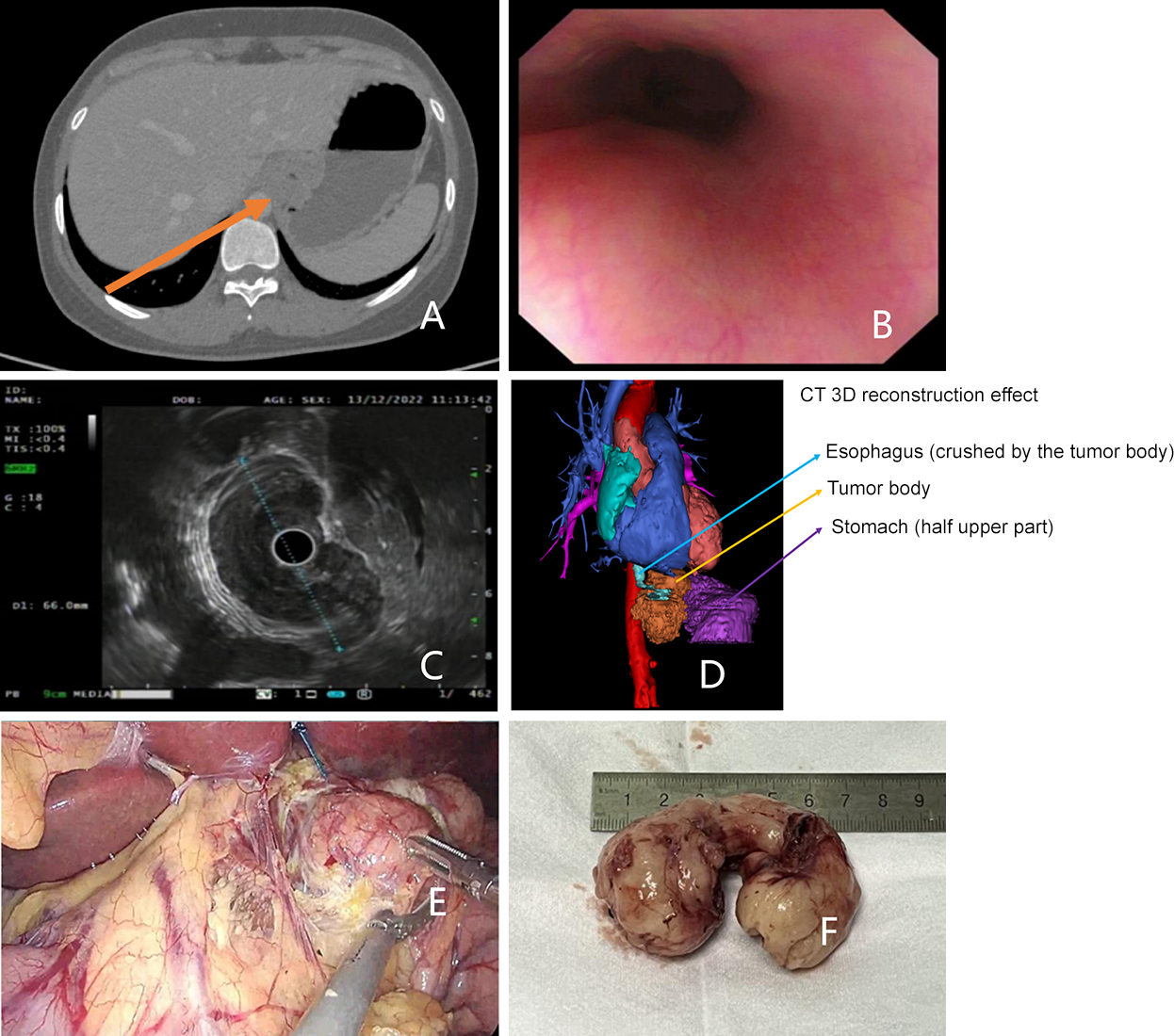
| Gastric stromal tumor | Per-multi-cavity-channel super minimally invasive resection | Peroral insertion of the gastroscope to perform the operation through a natural channel, the percutaneous puncture channel allowing the laparoscope to be inserted, in order to resect a gastric stromal tumor by the combination of the two endoscopes. |
| Early gastric cancer | Per-multi-cavity-channel super minimally invasive resection | Peroral insertion of the gastroscope to perform the operation through a natural channel, the percutaneous puncture channel allowing the laparoscope to be inserted, in order to resect the early gastric cancer foci and the D1 lymph nodes station by the combination of the two endoscopes. |
| Early colorectal cancer | Per-multi-cavity-channel super minimally invasive resection | Peroral insertion of the enteroscope to perform the operation through a natural channel, in order to resect the early colorectal cancer foci, the percutaneous puncture channel allowing the laparoscope to enter to carry out assisted resection and suture |
| Colorectal large polyp | Per-multi-cavity-channel super minimally invasive resection | Peroral insertion of the enteroscope to perform the operation through a natural channel, in order to resect the early colorectal cancer foci, the percutaneous puncture channel allowing the laparoscope to enter to carry out assisted resection and suture |
| Esophageal large muscularis propria mass | Per-multi-cavity-channel super minimally invasive resection | Peroral insertion of the gastroscope to perform the operation through a tunnel channel, in order to dissect the muscularis propria mass in the tunnel, the percutaneous puncture channel allowing the thoracoscope to enter to carry out assisted resection and suture |
| Biliary stone | Per-multi-cavity-channel super minimally invasive extract | Surgery using a percutaneous puncture channel to insert the laparoscope, and the natural channel of the bile duct to insert the choledochoscope, and combining the two endoscopes for the extraction of a biliary stone |
References
Chapter 4 Common Super Minimally Invasive Surgery Operations
4.1 Super Minimally Invasive Closure
4.1.1 SMIS Wound Closure Method
4.1.2 Hot-Spot Issues and Progress in the Search for a Consensus
4.2 Super Minimally Invasive Surgery for the Prevention and Therapy of Gastrointestinal Bleeding
4.2.1 Endoscopic Common Super Minimally Invasive Hemostatic Method
4.2.2 Hot-Spot Issues in the Consensus and Research Progress
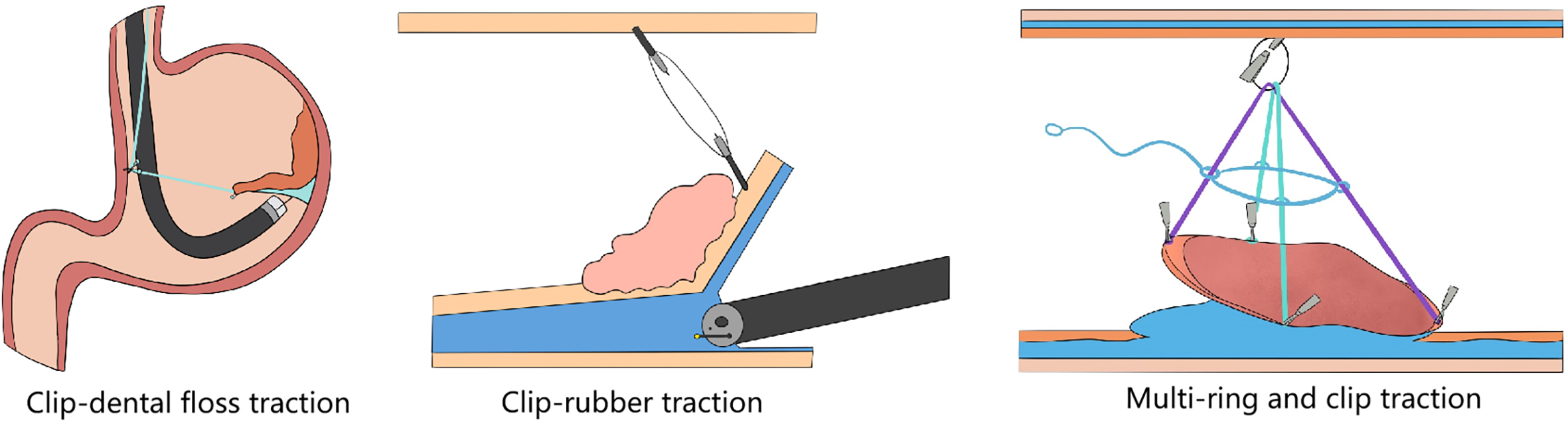
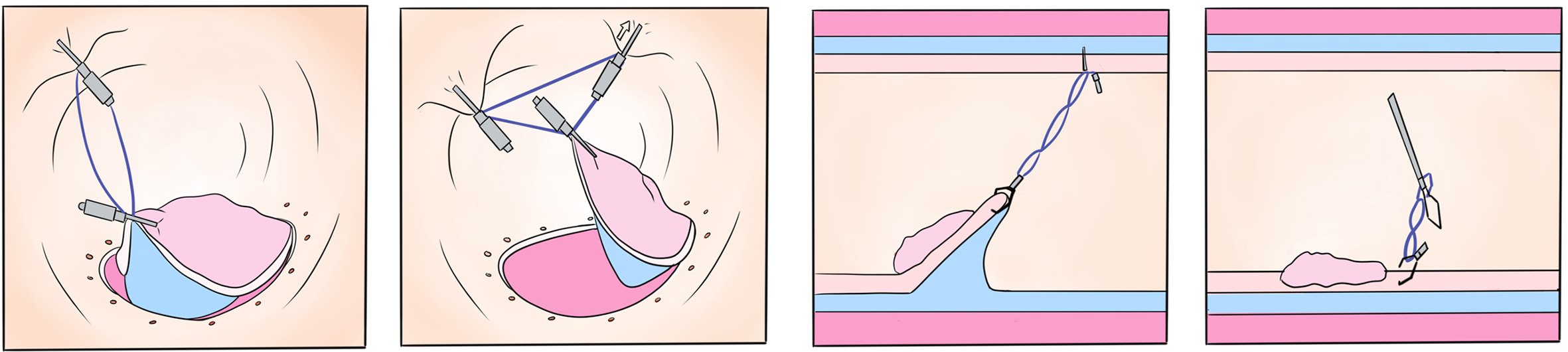
4.3 Super Minimally Invasive Auxiliary Traction Method
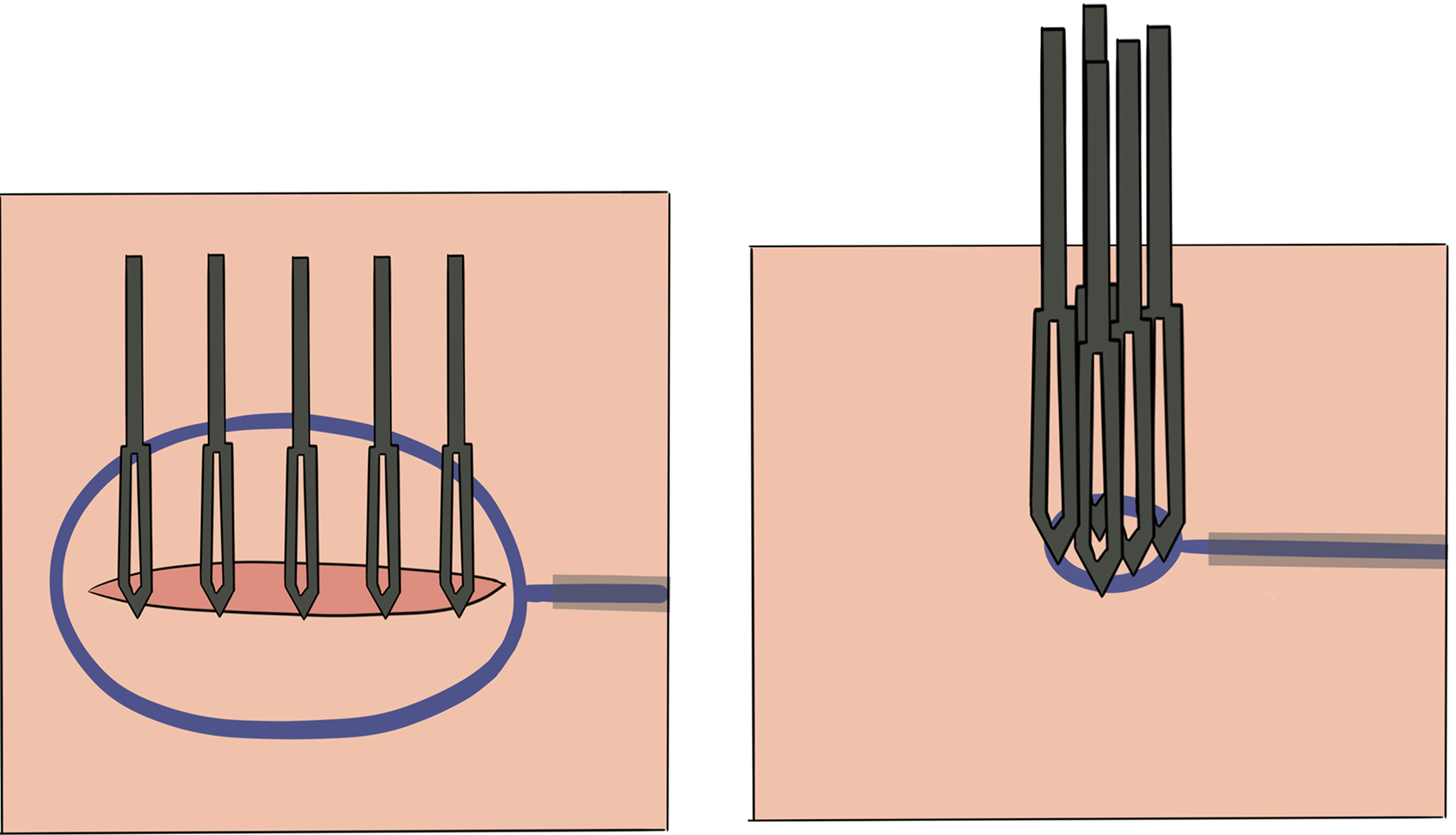
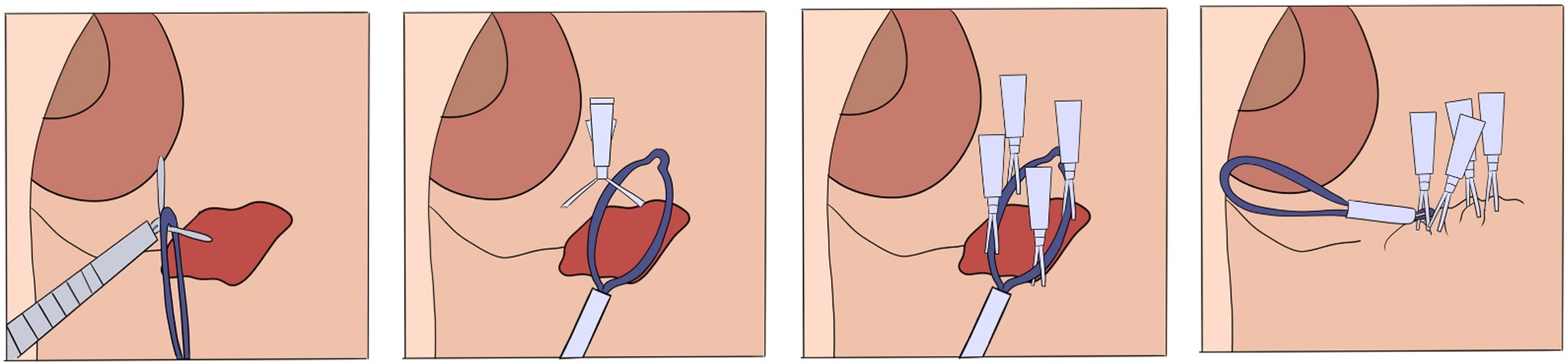
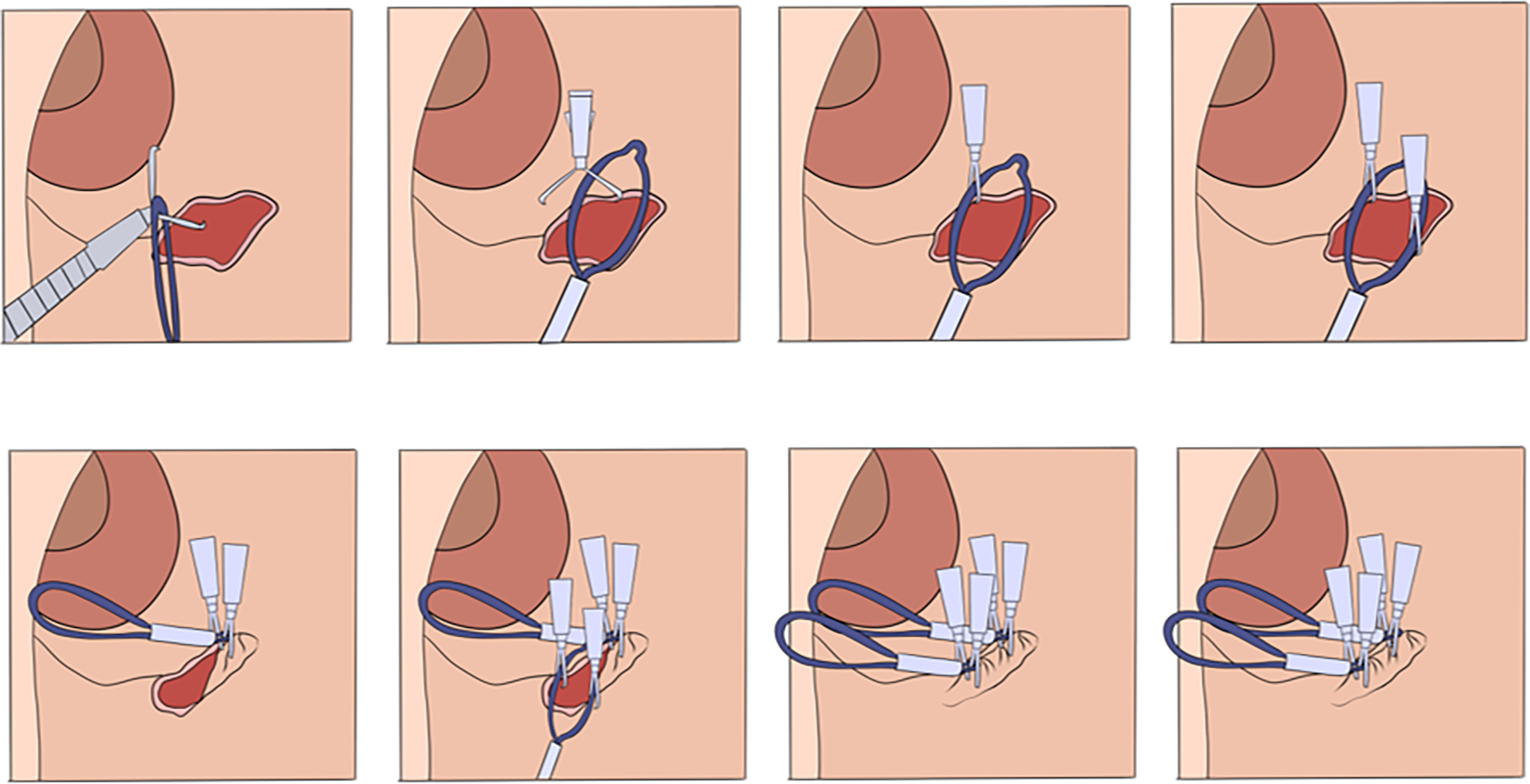
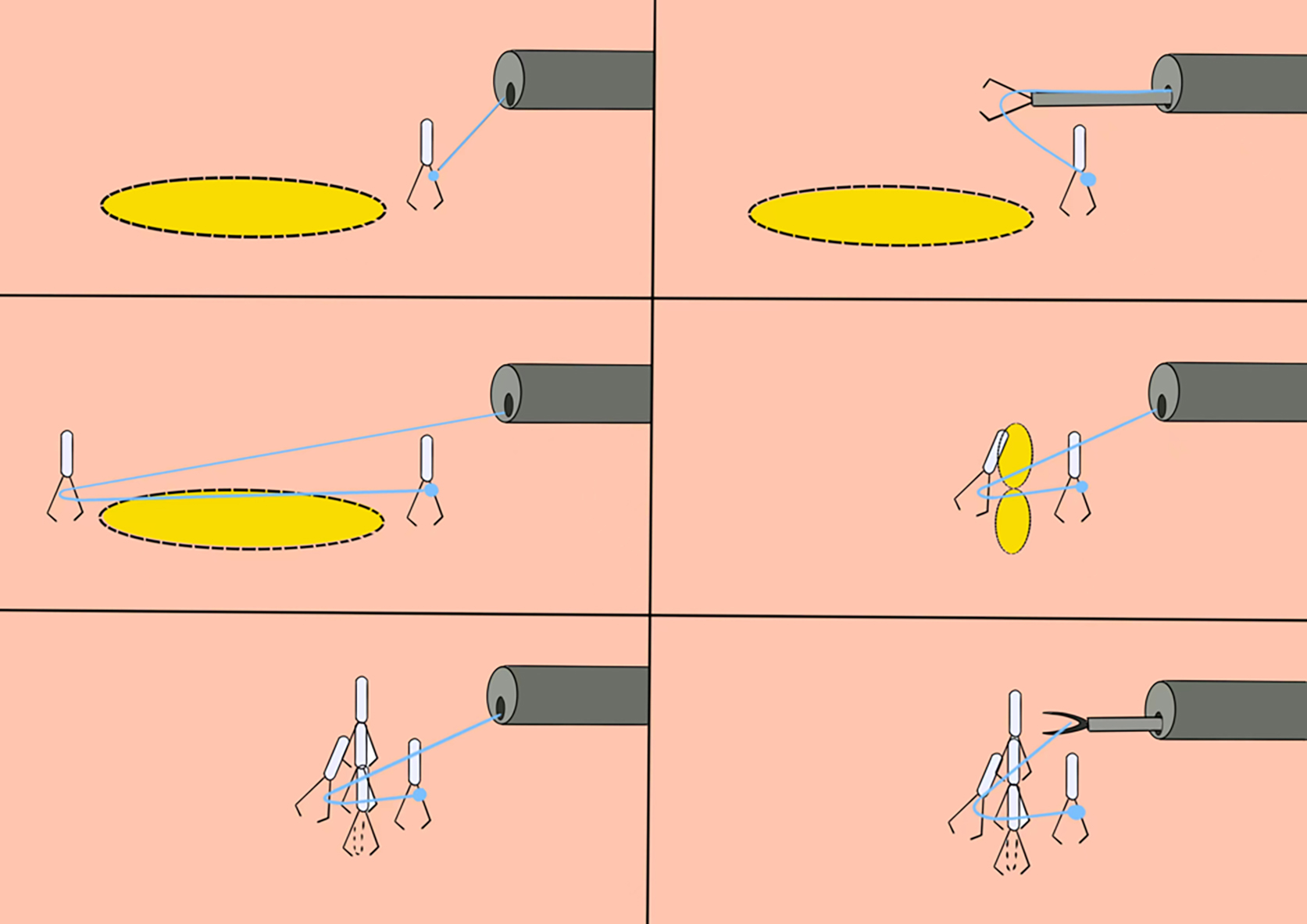
4.3.1 Clip–Thread Combined Traction Method
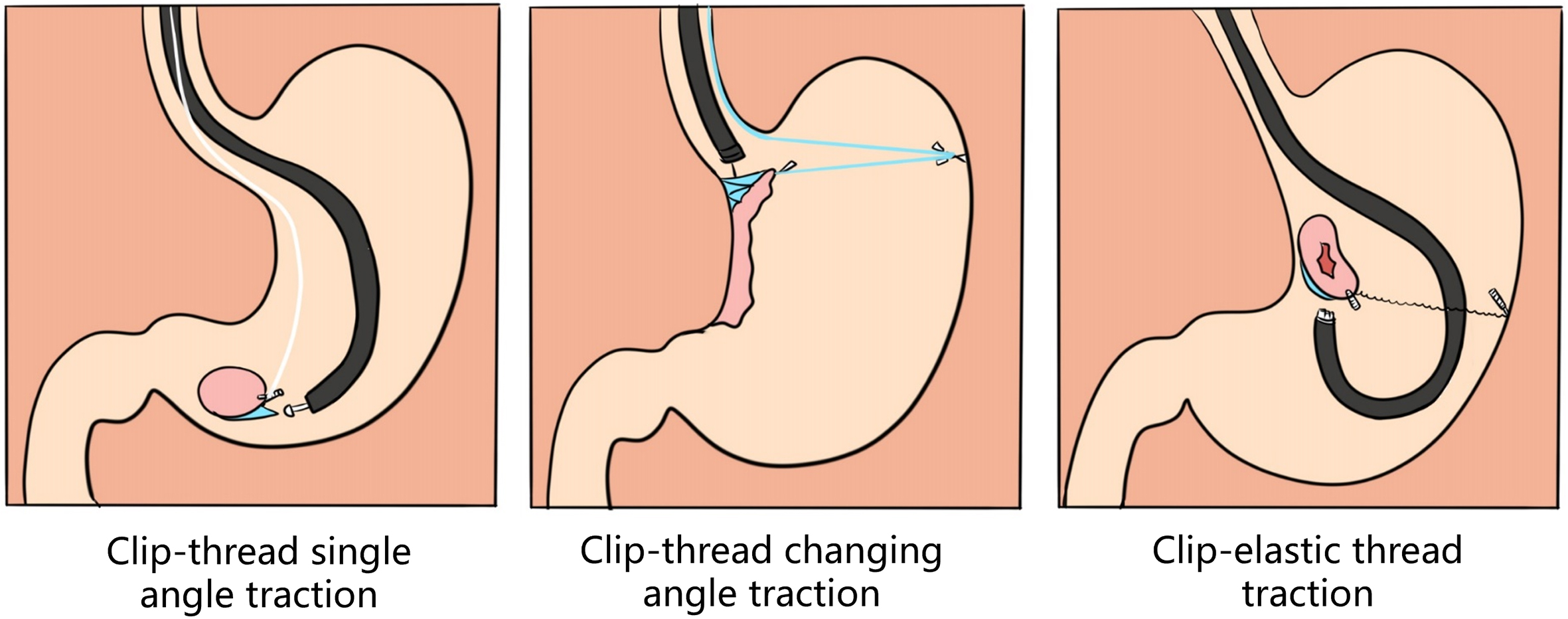
4.3.2 Clip–Elastic Ring Combined Traction Method
4.3.3 Other Combinations
4.3.4 Hot-Spot Issues in the Consensus and Research Progress
References
Chapter 5 Conditions for Performing Super Minimally Invasive Surgery
5.1 Site and Anesthesia Rules for Super Minimally Invasive Surgery

5.1.1 Site Facility
5.1.2 Anesthesia Rules for Super Minimally Invasive Surgery
5.2 Manning and Requirements for Performing Super Minimally Invasive Surgery
5.2.1 Surgeon
5.2.2 Anesthetist
5.2.3 Nurse
5.2.4 Operating Room Assistant
5.2.5 Operating Room Head Nurse
5.2.6 Cleaner
5.2.7 Operation Room Technician
5.2.8 Pathologist
5.3 Instruments and Parameters of Super Minimally Invasive Surgery
5.3.1 Electrosurgical Device

5.3.2 Surgical Equipment for Endoscopic Therapy
5.4 Common Instruments and Articles for Super Minimally Invasive Surgery
5.5 Standardized Operation and Management of the Cleaning and Disinfection of Gastroendoscopes
| Surgical method | Instrument | Mode | Device power (W) | Standard electric coagulation index | Argon flow control (l/min) | Treatment time control (second/time) |
| Marking | DualKnife | Forced | 20–30 or 20 | |||
| Arc knife | APC | 0.5 | ||||
| Mucosal resection | DualKnife | Endocut effect 3 | 80–120 | |||
| Mucosal dissection | DualKnife or IT or triangle knife | Endocut effect 3 | 80–120 | |||
| Vascular pretreatment | IT knife | Forced | 30 –50 | |||
| Hemostat | Soft | 50–80 | ||||
| Intraoperative hemorrhage | Hemostat | Soft | 50–80 or 30 | |||
| Arc knife | APC | 1.0 | ||||
| Wound treatment | Hemostat | Soft | 50–80 or 25 | |||
| Arc knife | APC | 1.0 | ||||
| Endoscopic argon ionization coagulation | Arc knife | Endocut | 45–60 | A40-50 | 2–3 | 1–3 |
References
Chapter 6 Standard Process of Super Minimally Invasive Surgery
6.1 Informed Consent Prior to Super Minimally Invasive Surgery
6.1.1 Legal Basis and Moral Consideration of the Informed Consent
6.1.2 The Contents and Requirements of Super Minimally Invasive Surgery
6.1.3 Practical Implementation of Informed Consent in Super Minimally Invasive Surgery
6.1.4 Postoperative Follow-Up Visit and Feedback
6.1.5 Difficulties and Strategy of Informed Consent in Super Minimally Invasive Surgery
6.2 Preoperative Conversation Skills in Super Minimally Invasive Surgery
6.2.1 Patient Psychological Profiling and Intervention of Super Minimally Invasive Surgery
6.2.2 Doctor–Patient Communication in Super Minimally Invasive Surgery
6.2.3 Information About Super Minimally Invasive Surgery (Surgical Purpose, Surgical Risk and Special Condition Inform)
6.2.4 Example of Informational Conversation on Super Minimally Invasive Surgery
6.2.5 Complication Management Principle
6.3 Standards for the Surgical Record of Clinical Cases
6.3.1 Basic Requirements for the Surgical Record
6.3.2 Specific Contents of the Surgical Record in Super Minimally Invasive Surgery
6.3.3 Postoperative Treatment and Medical Order
6.3.4 Notice and Follow-Up Visit
6.3.5 Writing Norm and Notice
6.3.6 Specific Writing Skills
6.4 Perioperative Diagnosis and Treatment Criteria
6.4.1 Preoperative Preparation
6.4.2 Intraoperative Operation
6.4.3 Postoperative Nursing
6.4.4 Prevention of Complications
6.4.5 Management of Follow-Up Visits
References
Chapter 7 Preoperative Preparation and Treatment of Complications in Super Minimally Invasive Surgery
7.1 Preparation Before the Endoscopic Operation
7.1.1 Preparation of the Endoscopic Operation of the Upper Digestive Tract
7.1.2 Preparation of the Endoscopic Operation of the Lower Digestive Tract
7.1.3 Preparation Before an Enteroscopic Operation
7.1.4 Preparation Before an Operation by Duodenoscopy
7.1.5 Preparation Before the Ultrasonic Endoscopy Examination
7.1.6 Preparation Before the SpyGlass Operation
7.1.7 Hot-Spot Issues in the Consensus
7.2 Preoperative Preparation of the Patient for Super Minimally Invasive Surgery
7.2.1 Medical Preparation
7.2.2 Nursing Preparation
7.2.3 Hot-Spot Issues in the Consensus
7.3 Wound Pre-Treatment and Infection Prevention in Super Minimally Invasive Surgery
7.3.1 Wound Pre-Treatment Plan in Super Minimally Invasive Surgery
7.3.2 Antibiotic Application in Super Minimally Invasive Surgery
7.3.3 Hot-Spot Issues in the Consensus
7.4 Prevention and Treatment of Intraoperative Complications in Super Minimally Invasive Surgery
7.4.1 Complication Prevention and Treatment
7.4.2 Hot-Spot Issues in the Consensus
7.5 Prevention and Treatment of Postoperative Complications in Super Minimally Invasive Surgery
7.5.1 Complication Prevention and Treatment
7.5.2 Hot-Spot Issues in the Consensus
7.6 Postoperative Nursing in Super Minimally Invasive Surgery
7.6.1 Peroral Super Minimally Invasive Surgery
7.6.2 Psychological Nursing
7.6.3 Health Education
7.6.4 Transanal Super Minimally Invasive Surgery
7.6.5 Hot-Spot Issues in the Consensus
References
Part Two Specific Discussion of Super Minimally Invasive Surgery
Chapter 8 Super Minimally Invasive Surgery of Esophageal Diseases
8.1 Early Esophageal Carcinoma and Super Minimally Invasive Surgery
8.1.1 Introduction
| No. | Super Minimally Invasive Surgery (SMIS) | Technique | Past Name |
| 1 | Peroral super minimally invasive resection of an early esophageal carcinoma | Super minimally invasive non-full-thickness resection | Endoscopic submucosal dissection |
| Endoscopic submucosal dissection with traction | |||
| Cap-assisted endoscopic mucosal dissection | |||
| 2 | Per-tunnel super minimally invasive resection of an early esophageal carcinoma | Super minimally invasive non-full-thickness resection | Endoscopic tunnel submucosal dissection |
| Endoscopic submucosal dissection with traction | |||
| 3 | Peroral super minimally invasive stenosis treatment for early esophageal carcinoma | Super minimally invasive surgery of stenosis | Gastrointestinal endoscopic super minimally invasive esophageal surface skin transplantation |
| Endoscopic esophageal stenting |
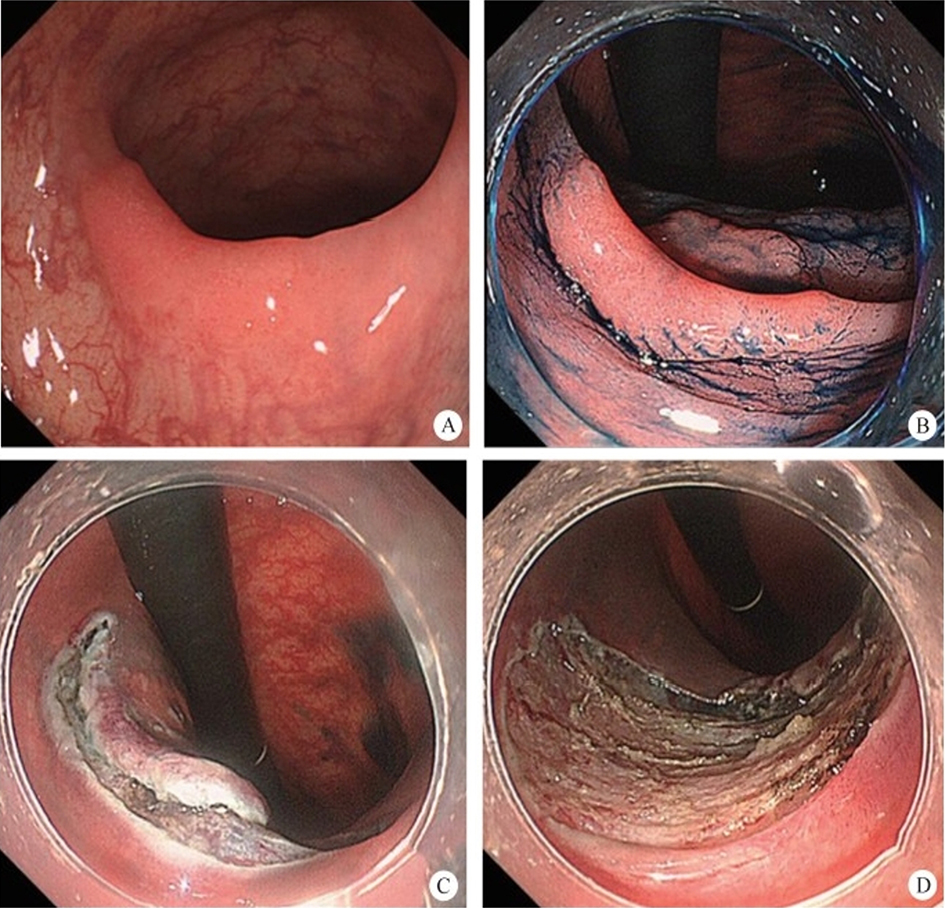
8.1.2 Peroral Super Minimally Invasive Surgery with Non-Full-Thickness Resection for the Treatment of Early Esophageal Carcinoma
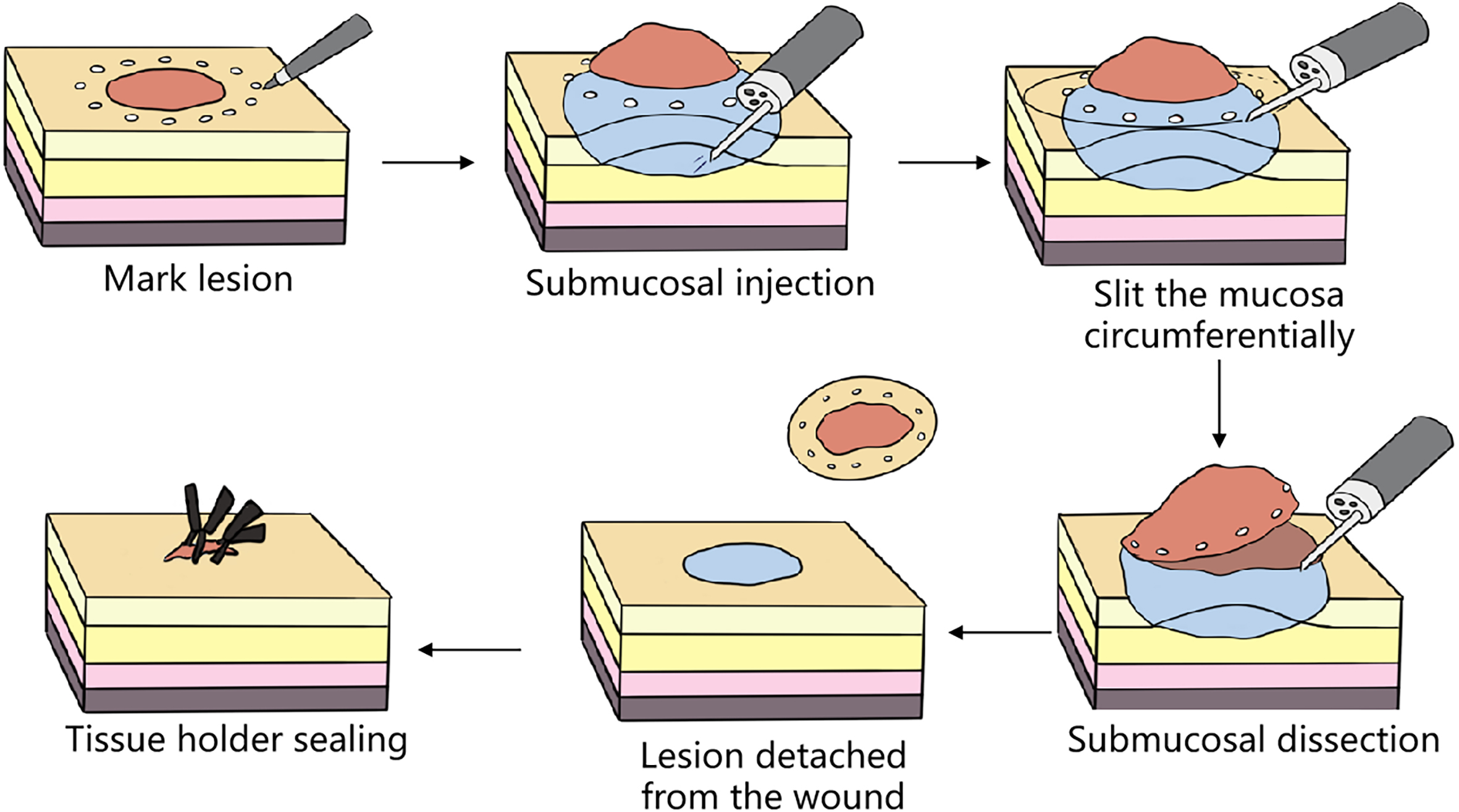
8.1.2.1 Endoscopic Submucosal Dissection (ESD)
8.1.2.2 Endoscopic Submucosal Dissection with Traction
After an adequate preoperative evaluation, an improvement in nutritional status, and the signing of informed consent for surgery, the patient underwent a peroral super minimally invasive resection of an early esophageal carcinoma (Refer to video 8.1, Peroral super minimally invasive resection for early esophageal carcinoma (See online resources)).
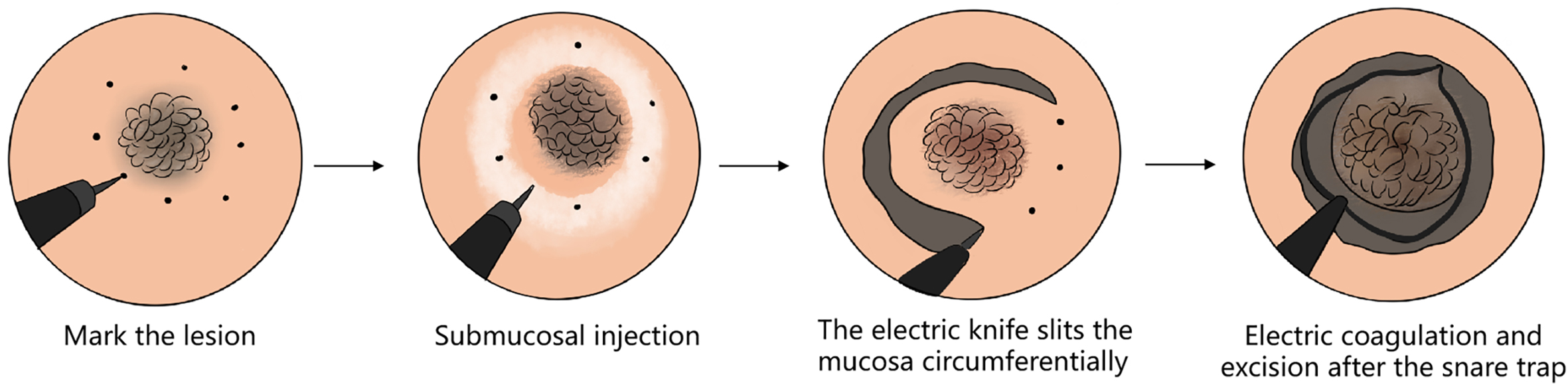
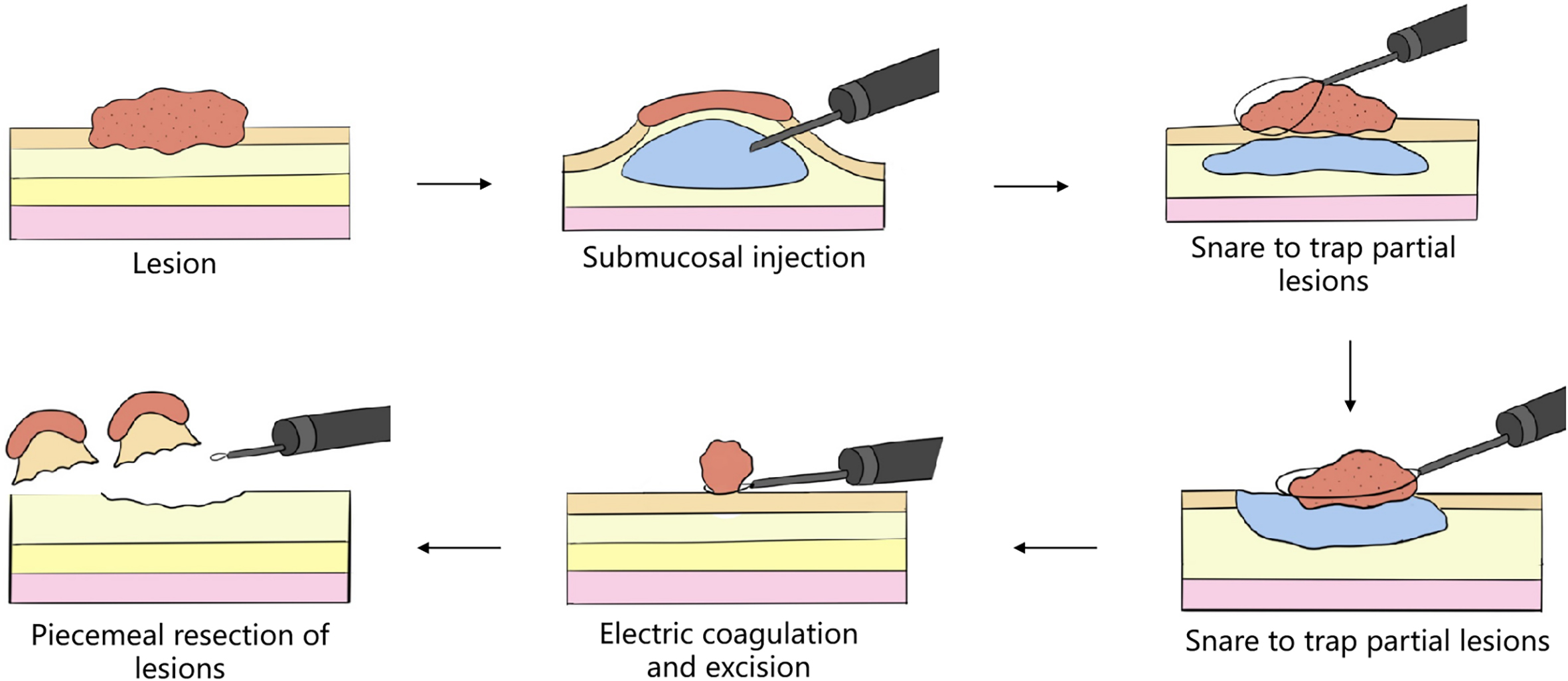
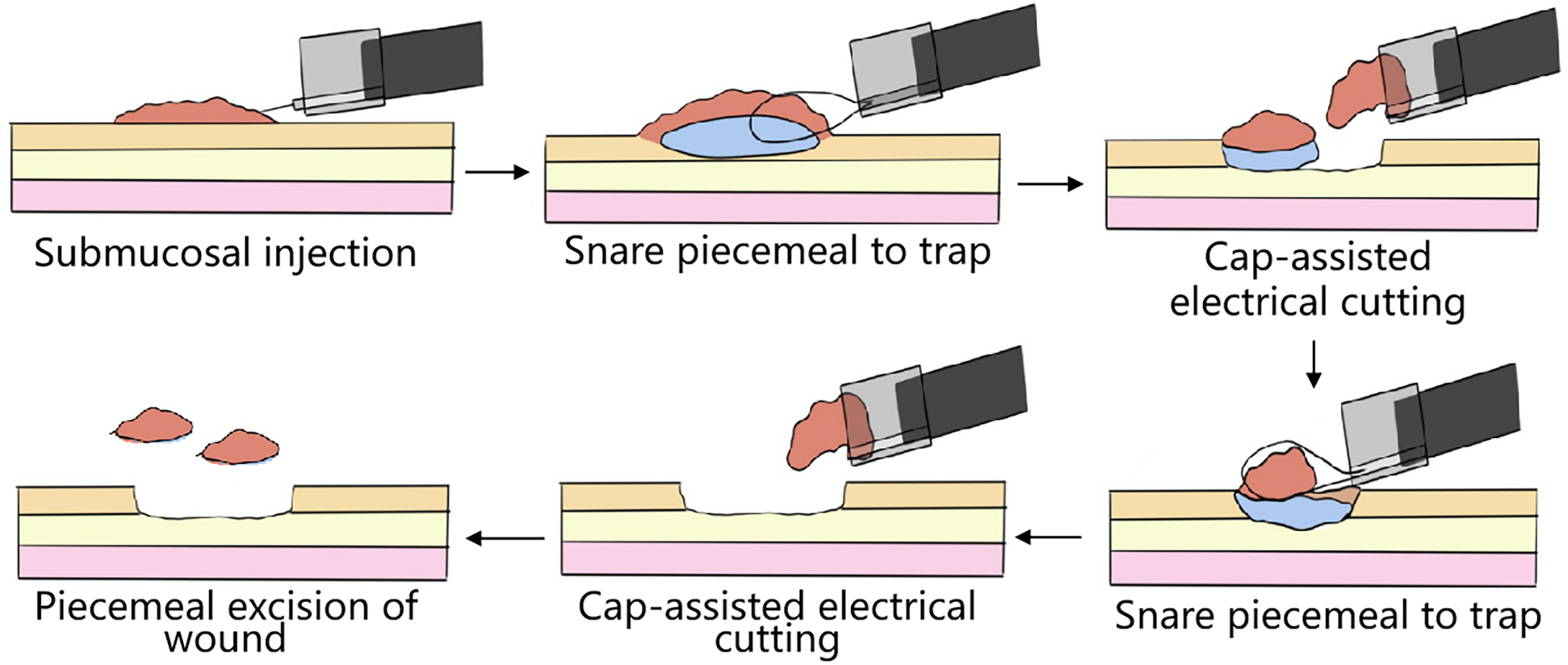
8.1.2.3 Cap-Assisted Endoscopic Mucosal Resection
8.1.3 Non-Full-Thickness Resection of Early Esophageal Carcinoma by Per-Tunnel Super Minimally Invasive Surgery
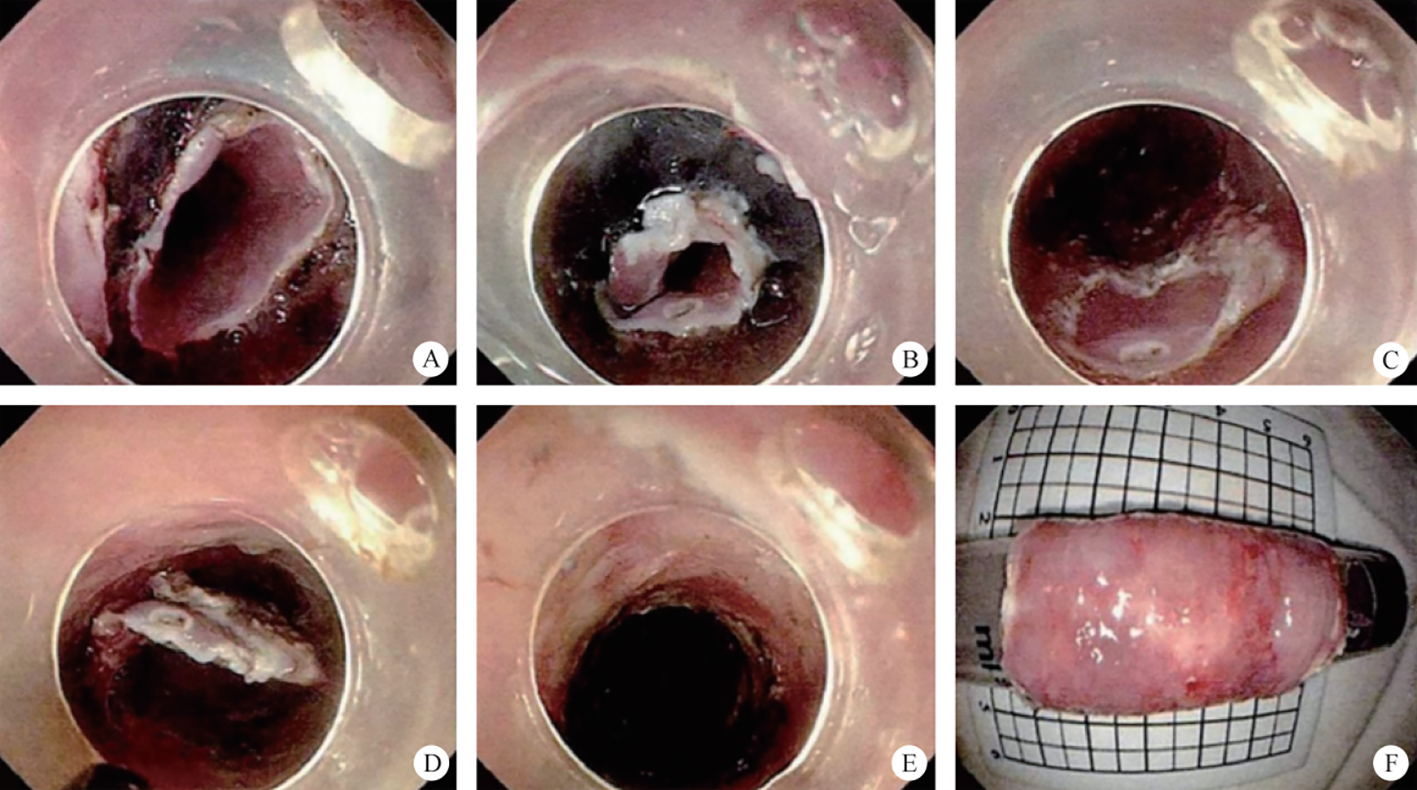
After full preoperative evaluation, improving nutrition condition and signing the surgery informed consent form, the early esophageal carcinoma per-single-tunnel channel SMIS resection was performed on the patient (Refer to video 8.2, Early esophageal carcinoma resection by super minimally invasive surgery through a tunnel channel (See online resources)).
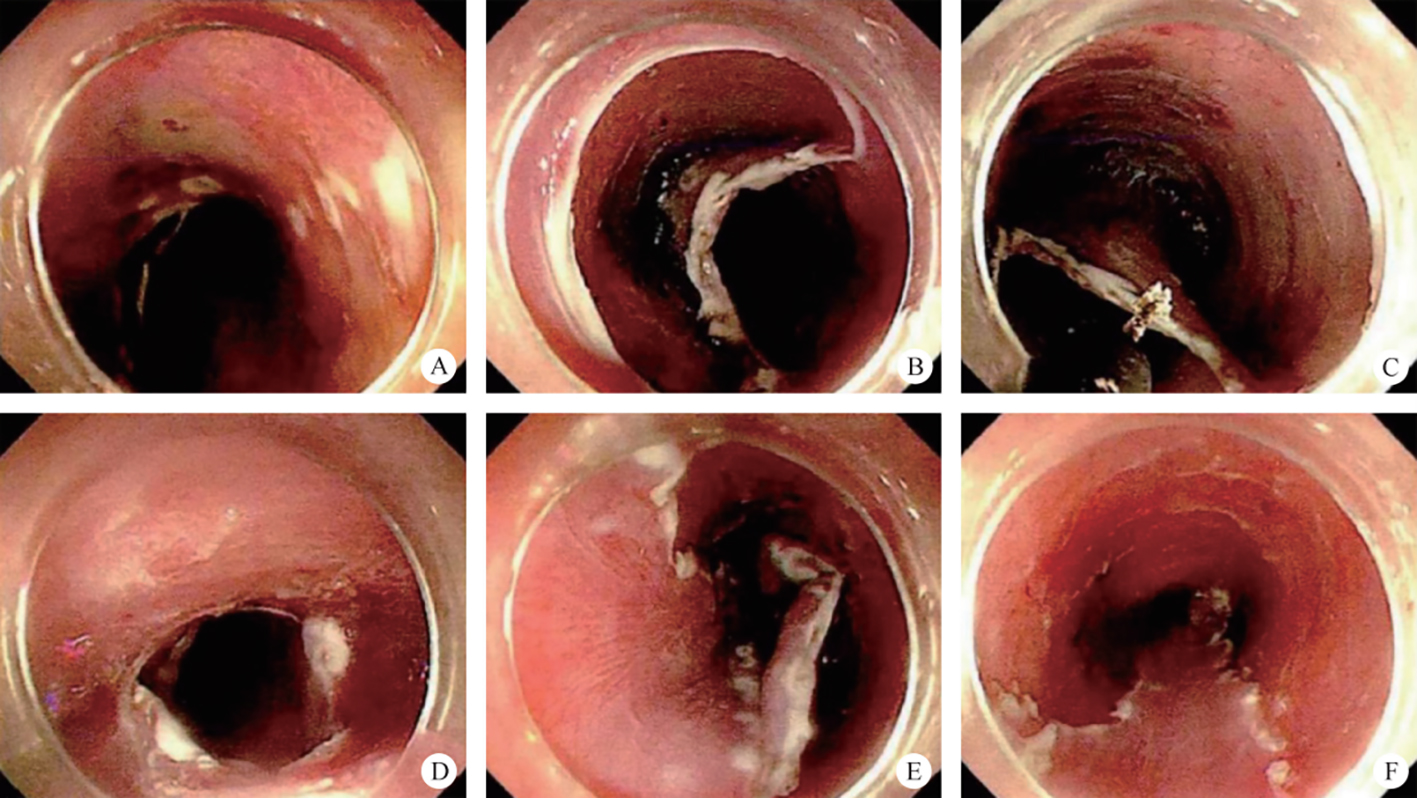
8.1.4 Esophageal Skin Grafting by Digestive Endoscopic Super Minimally Invasive Surgery
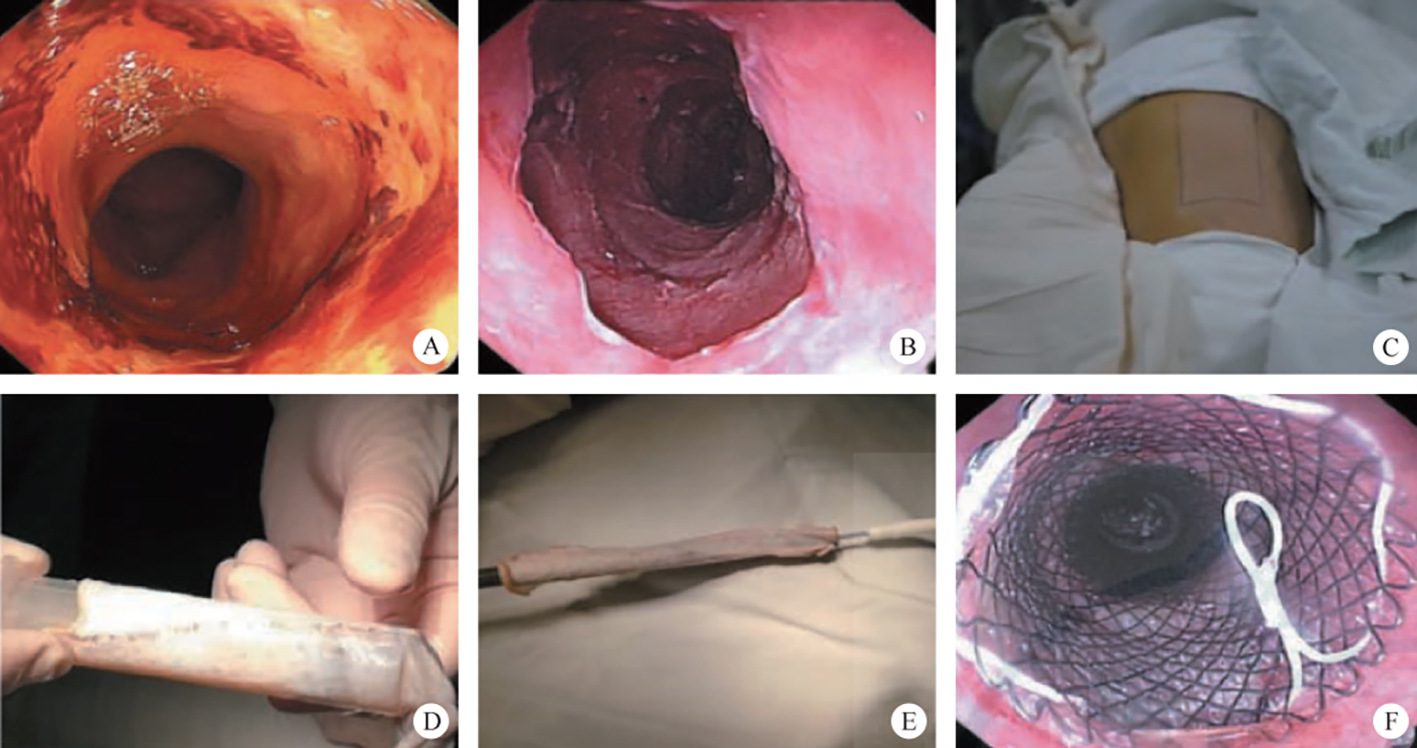
Refer to video 8.3, Digestive endoscopic super minimally invasive esophageal skin grafting surgery-1 (See online resources).
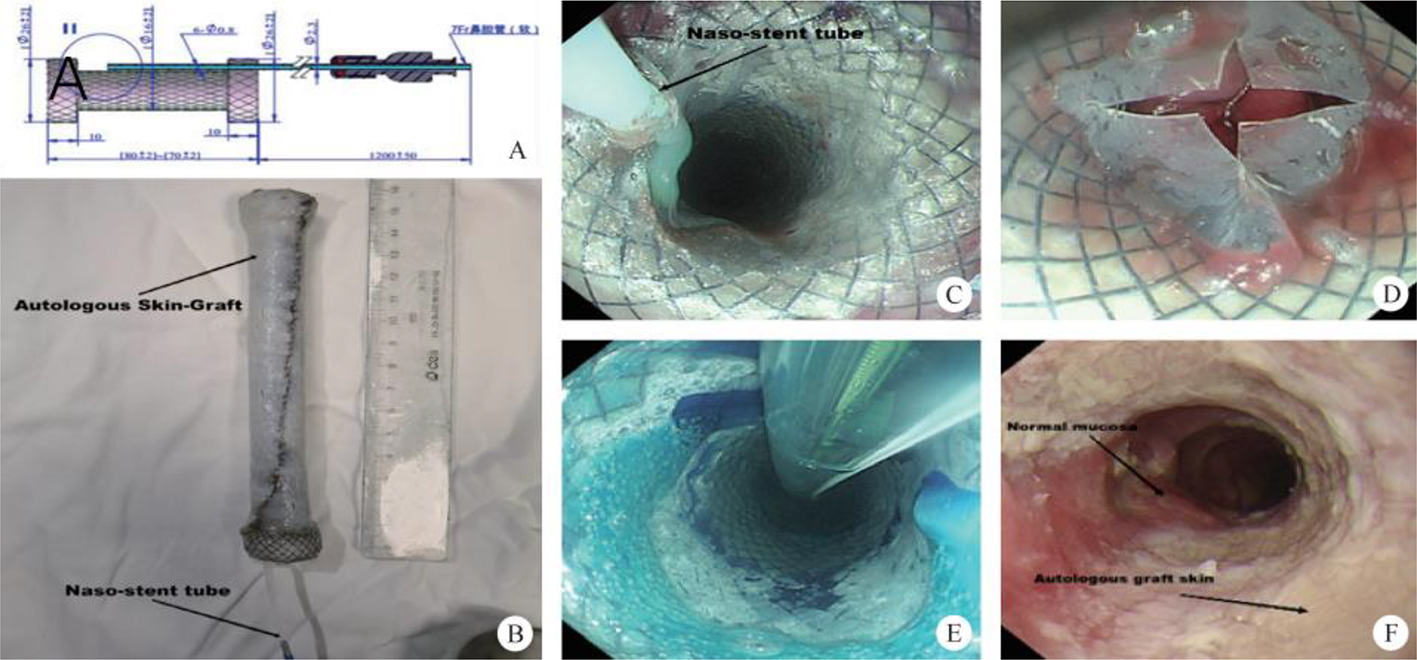
Refer to video 8.4, Digestive endoscopic super minimally invasive esophageal skin grafting surgery-2 (See online resources).
8.2 Super Minimally Invasive Surgery of Esophageal Subepithelial Lesions
8.2.1 General Introduction
| No. | Super Minimally Invasive Surgery (SMIS) | Technique | Past Name |
| 1 | Peroral super minimally invasive resection of esophageal subepithelial lesions | Super minimally invasive non-full-thickness resection | Endoscopic submucosal mass excavation |
| Endoscopic submucosal dissection | |||
| Endoscopic submucosal dissection with traction | |||
| Cap-assisted endoscopic mucosal resection | |||
| 2 | Peroral super minimally invasive resection of esophageal subepithelial lesions | Super minimally invasive full-thickness resection | Endoscopic subepithelial mass full-thickness resection |
| 3 | Per-tunnel super minimally invasive resection of esophageal subepithelial lesions | Endoscopic submucosal tumor resection by tunnel | Per submucosal tunnel endoscopic tumor resection |
| Resection of esophageal subepithelial lesions with traction | |||
| 4 | Per-multi cavity super minimally invasive resection of esophageal subepithelial lesions | Per multiple-cavity channel super minimally invasive resection | Multiple endoscopic combined therapy |
8.2.2 Peroral Super Minimally Invasive Resection of Esophageal Subepithelial Lesions
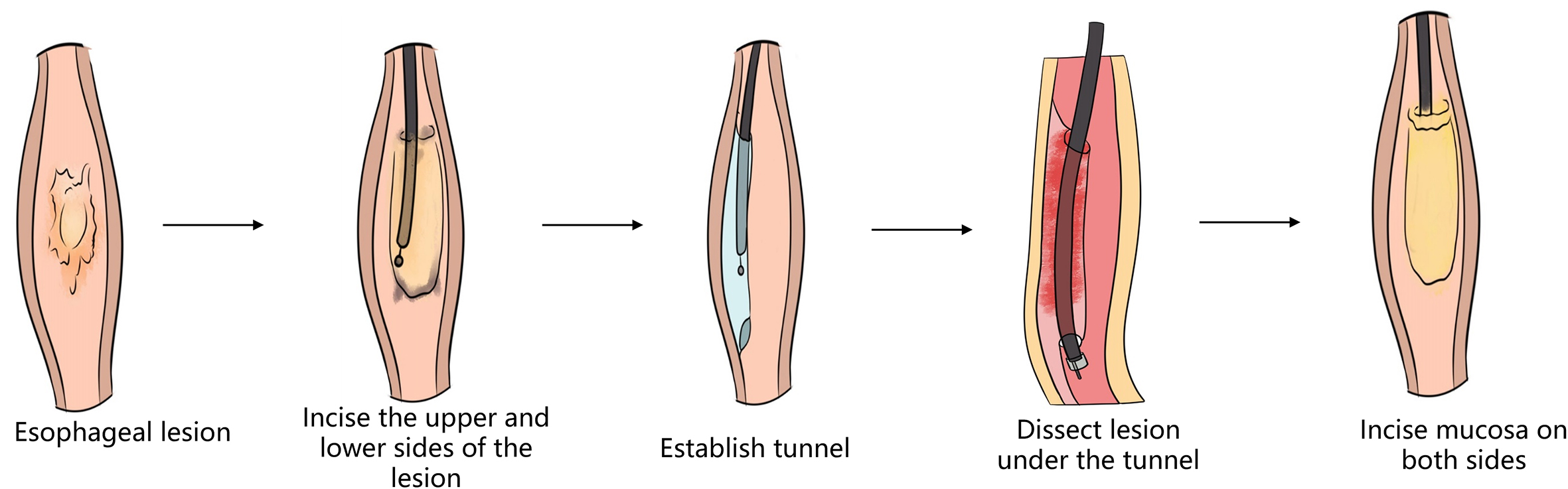
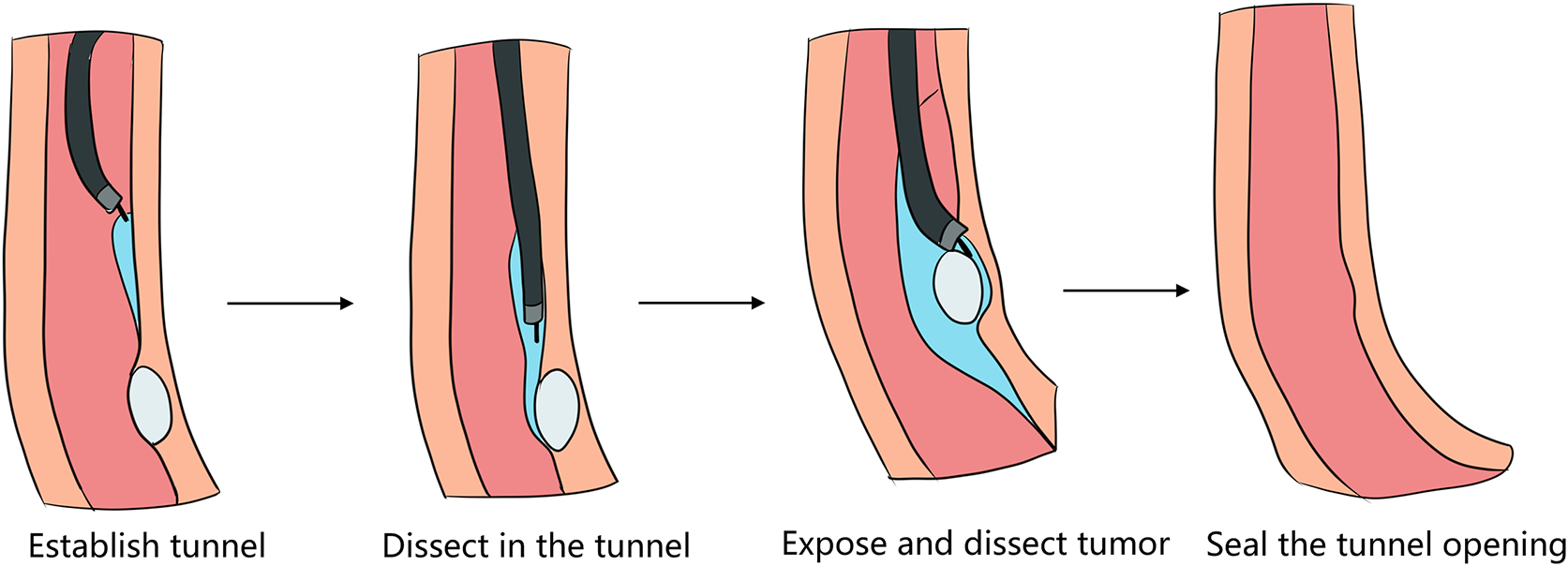
8.2.3 Per-Tunnel Super Minimally Invasive Resection of Esophageal Subepithelial Lesions
After full preoperative evaluation, improvement of the nutrition state and signing of surgery informed consent, the patient was performed peroral super minimally invasive resection of esophageal subepithelial lesions (Refer to video 8.5, Peroral super minimally invasive resection of esophageal subepithelial lesions through a tunnel channel (See online resources)).
8.2.4 Super Minimally Invasive Resection Per-Multi Cavity of Esophageal Subepithelial Lesions
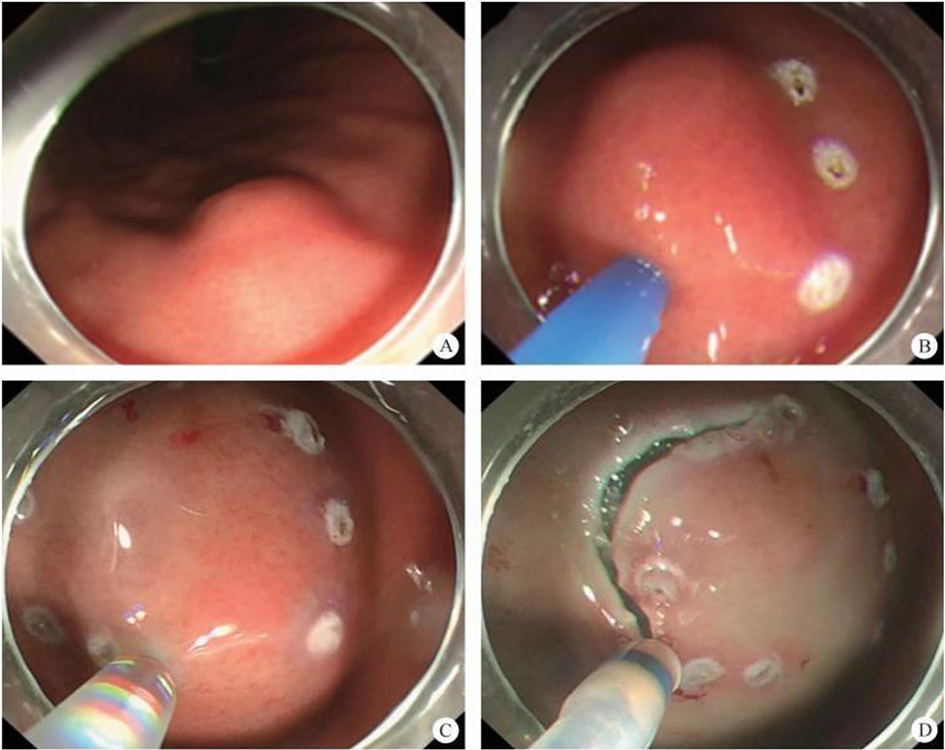
8.3 Super Minimally Invasive Radiofrequency Ablation for Intraepithelial Neoplasia
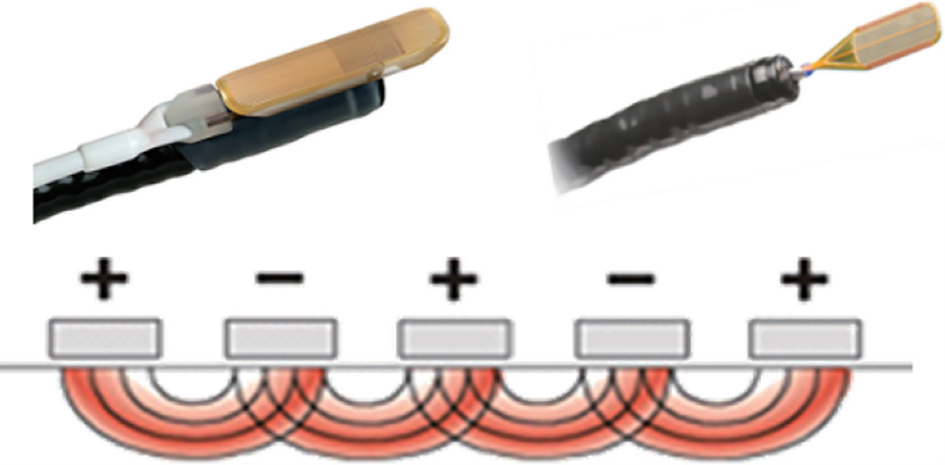
8.3.1 Principle of Radiofrequency Ablation
8.3.2 Indications and Contraindications of Super Minimally Invasive RFA Surgery

8.3.3 Preoperative Preparation
8.3.4 Surgical Operation and Skills
8.3.5 Postoperative Treatment
Refer to video 8.6, Super minimally invasive radiofrequency ablation of low grade intraepithelial neoplasia (See online resources).
8.3.6 Postoperative Follow-Up Visit
8.3.7 Hot-Spot Issues in the Consensus and Progress of the Study
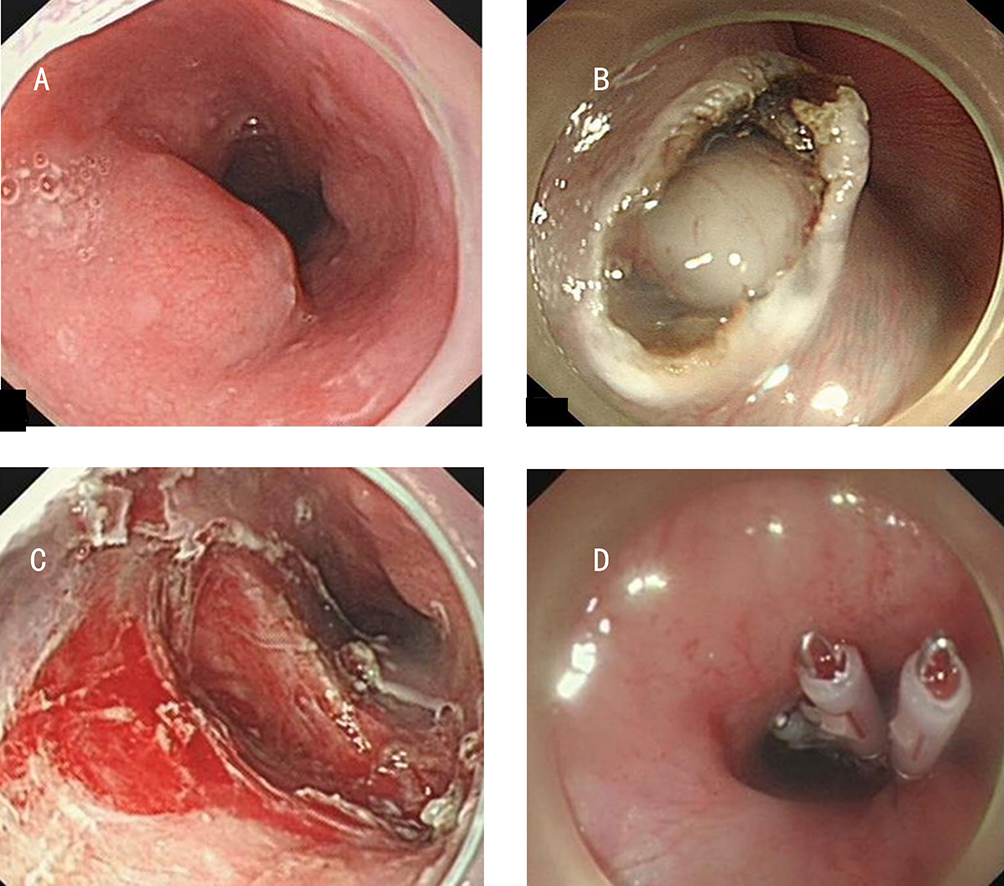
8.4 Super Minimally Invasive Surgery for Esophageal Stricture
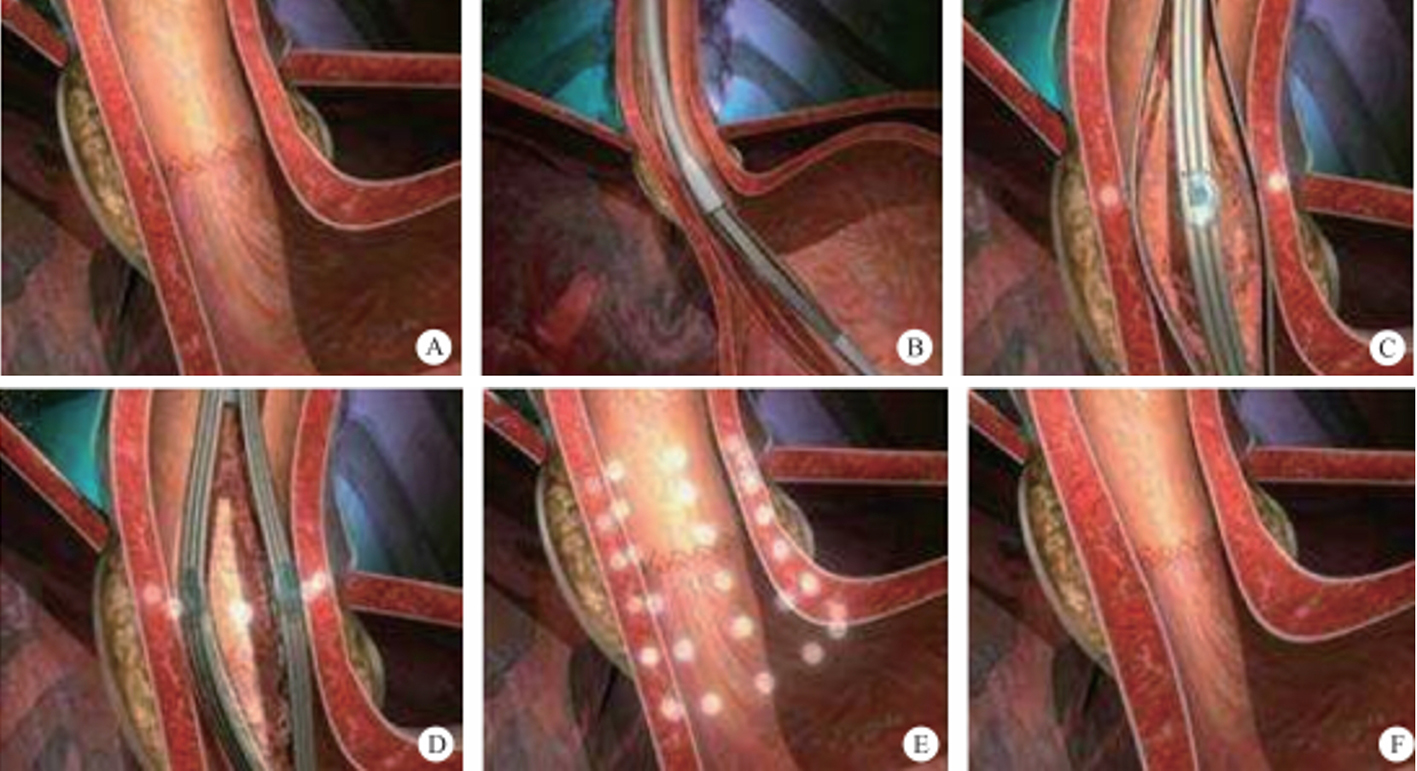
8.4.1 Esophageal Stenosis Peroral Super Minimally Invasive Incision + Submucosal Injection
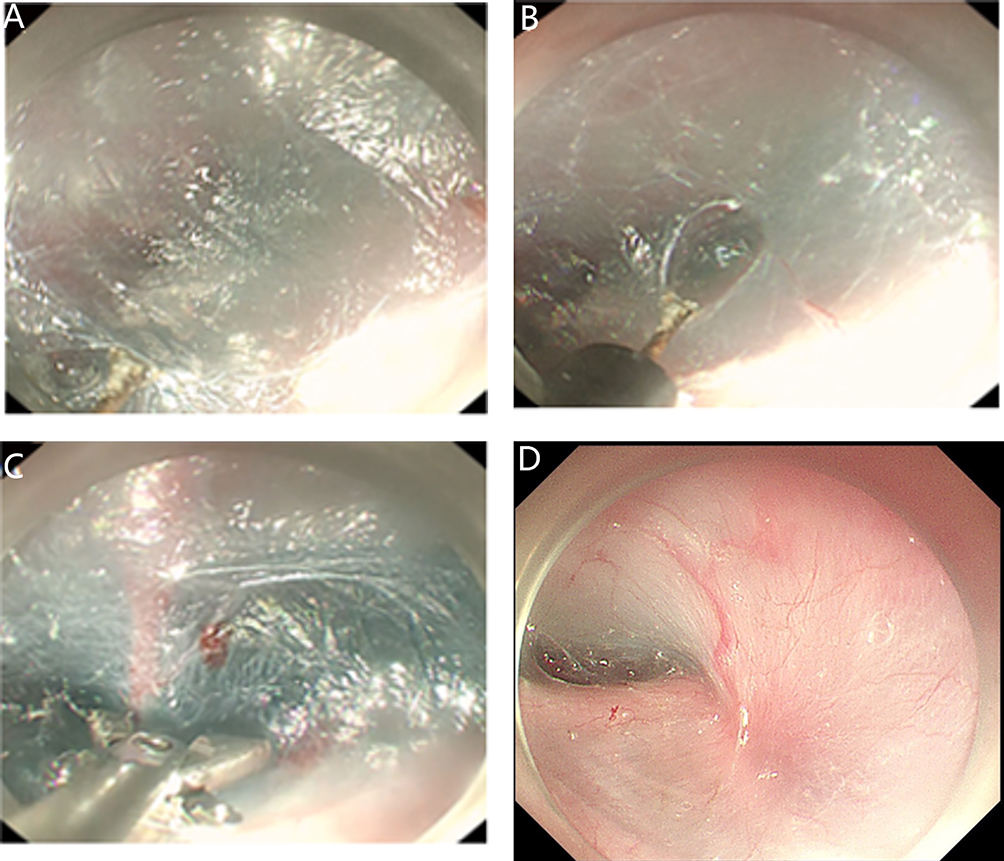
8.4.2 Peroral Super Minimally Invasive Dilation of Esophageal Stenosis
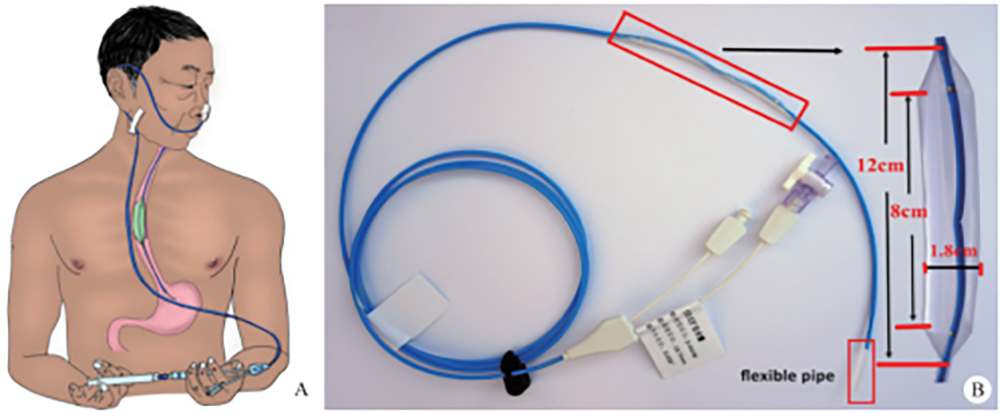
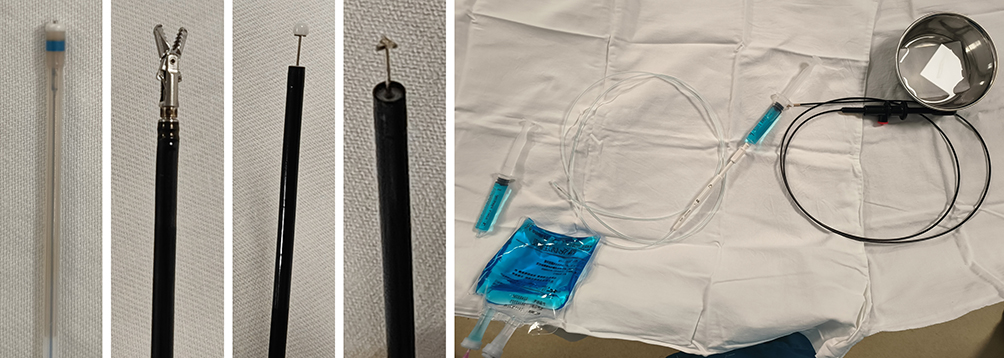
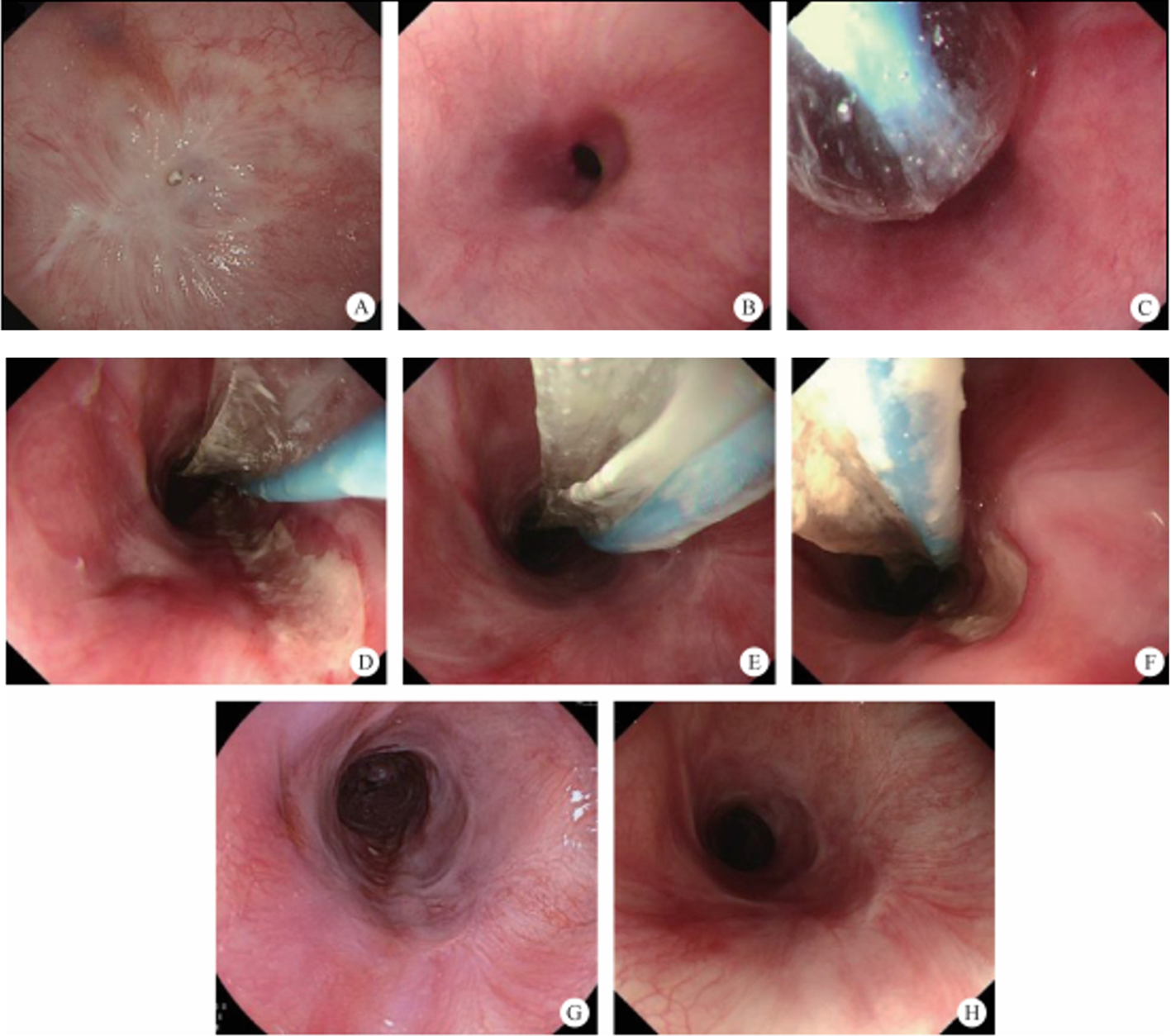
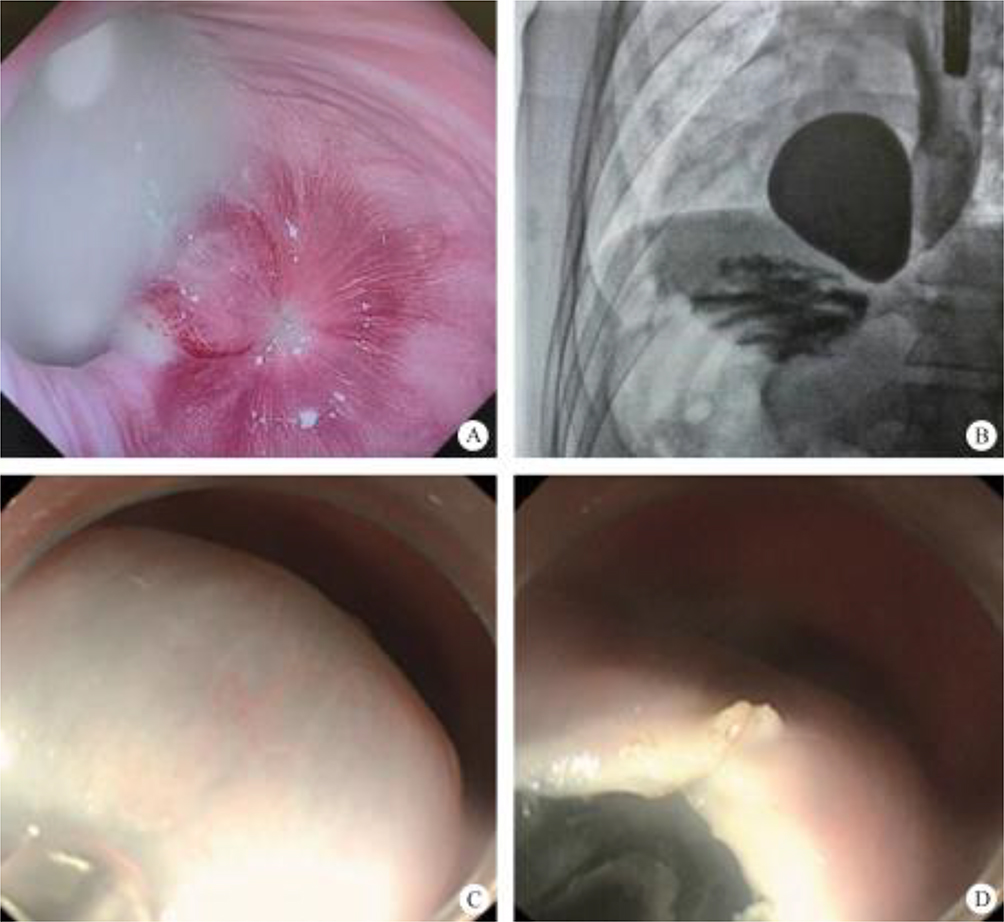
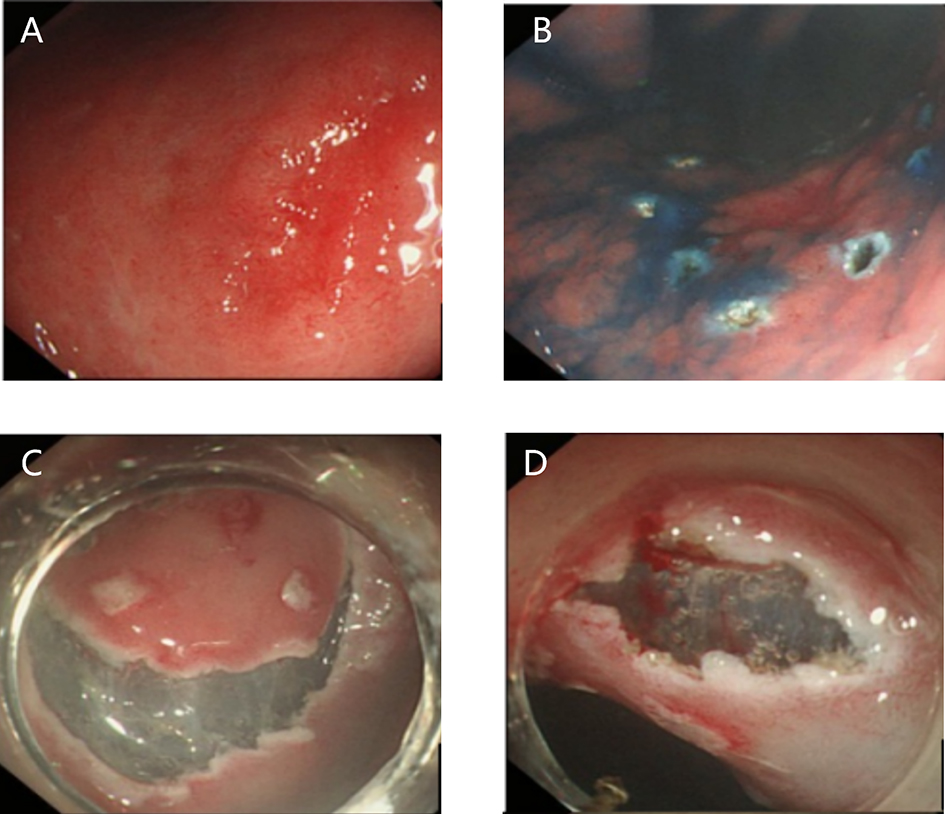
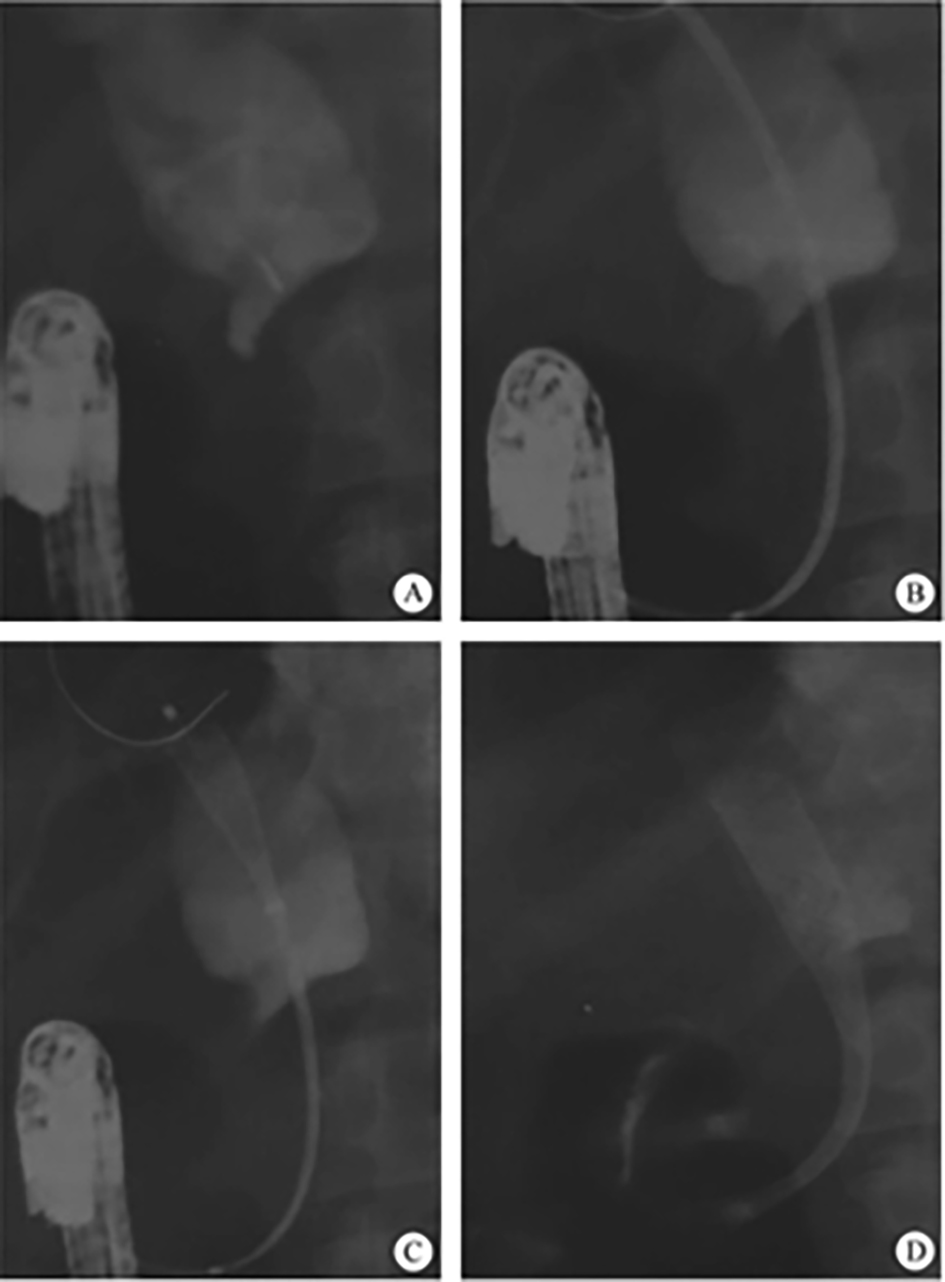
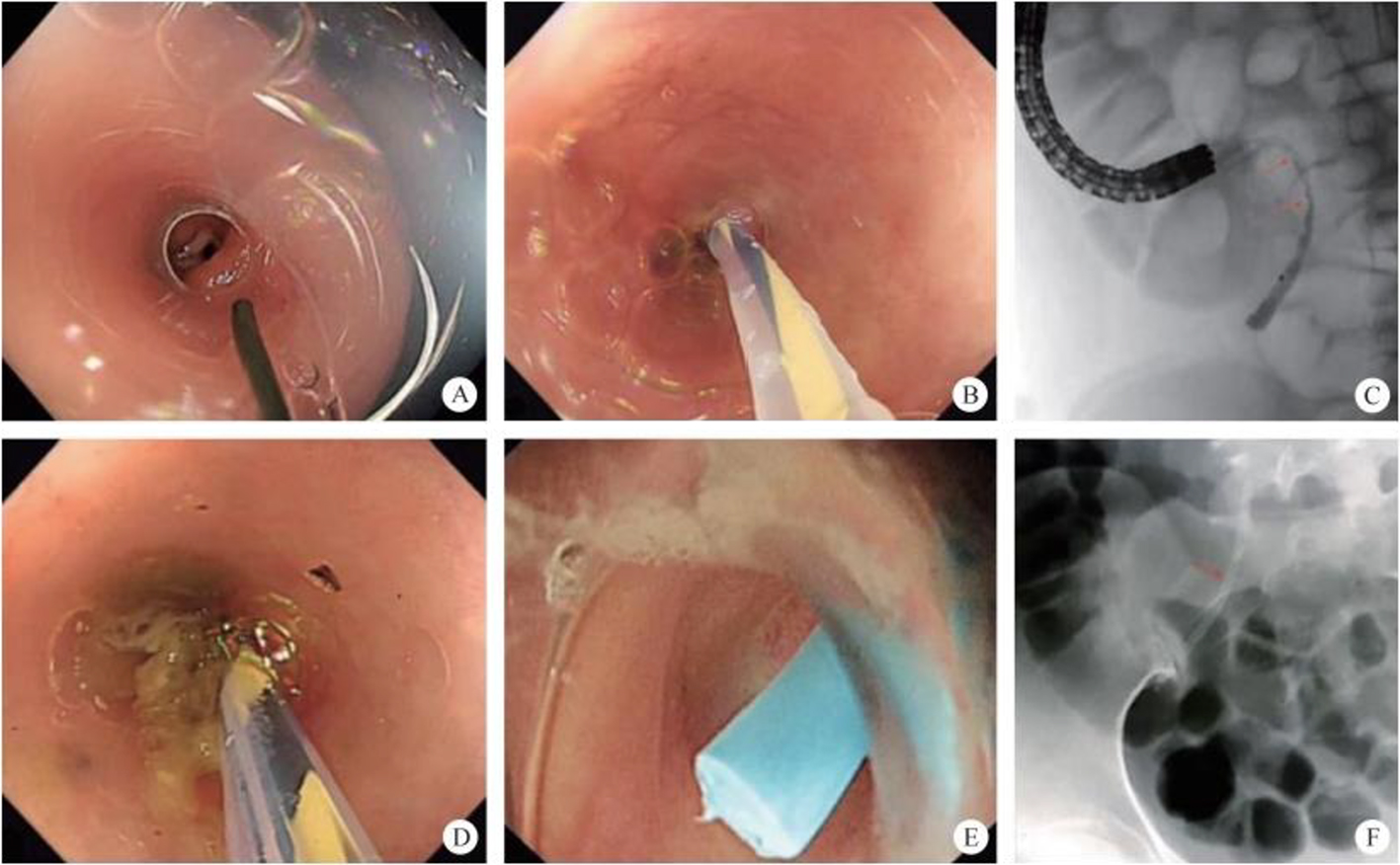
(2) Place in the balloon: the placement method is similar to that of the gastric retention tube, using liquid paraffin to lubricate the balloon, which must be slowly inserted along the selected nostril, asking the patient to make a swallowing movement. The balloon’s position must be adjusted under endoscopic observation, so as to ensure that the balloon is located in the middle part of the stenosis (figure 8.24A).

8.5 Super Minimally Invasive Surgery for Gastroesophageal Reflux Disease
8.5.1 Introduction
8.5.2 Peroral Super Minimally Invasive Radiofrequency Ablation to Cure Gastroesophageal Reflux Disease
8.5.3 Peroral Incisionless Fundoplication for Gastroesophageal Reflux Disease
8.5.4 Peroral Super Minimally Invasive Mucosa Resection for Gastroesophageal Reflux Disease
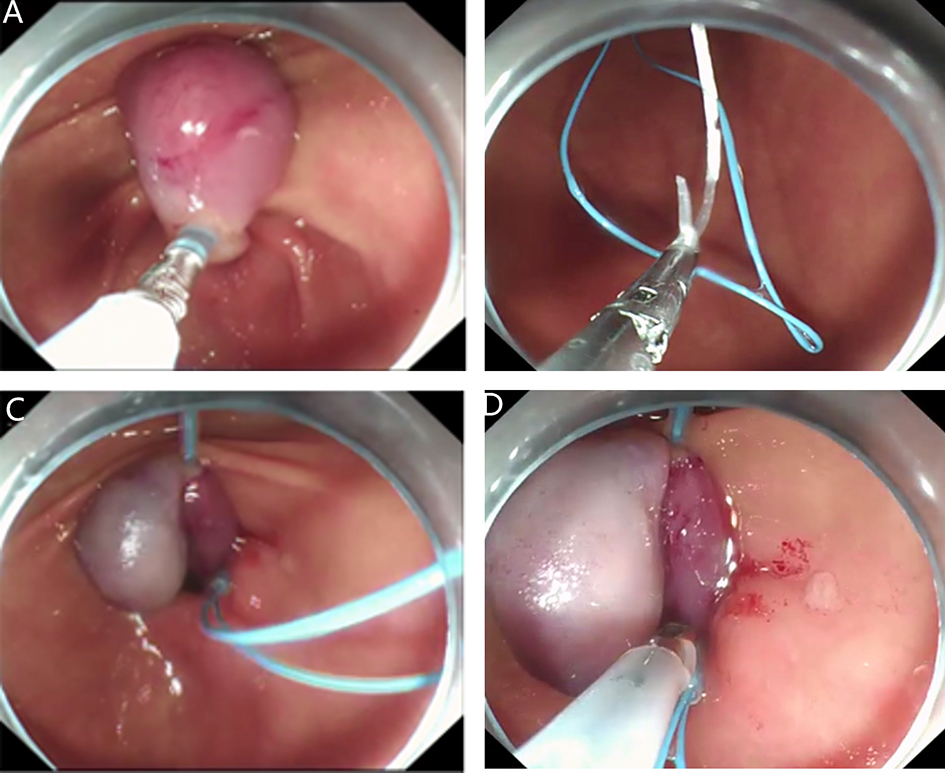
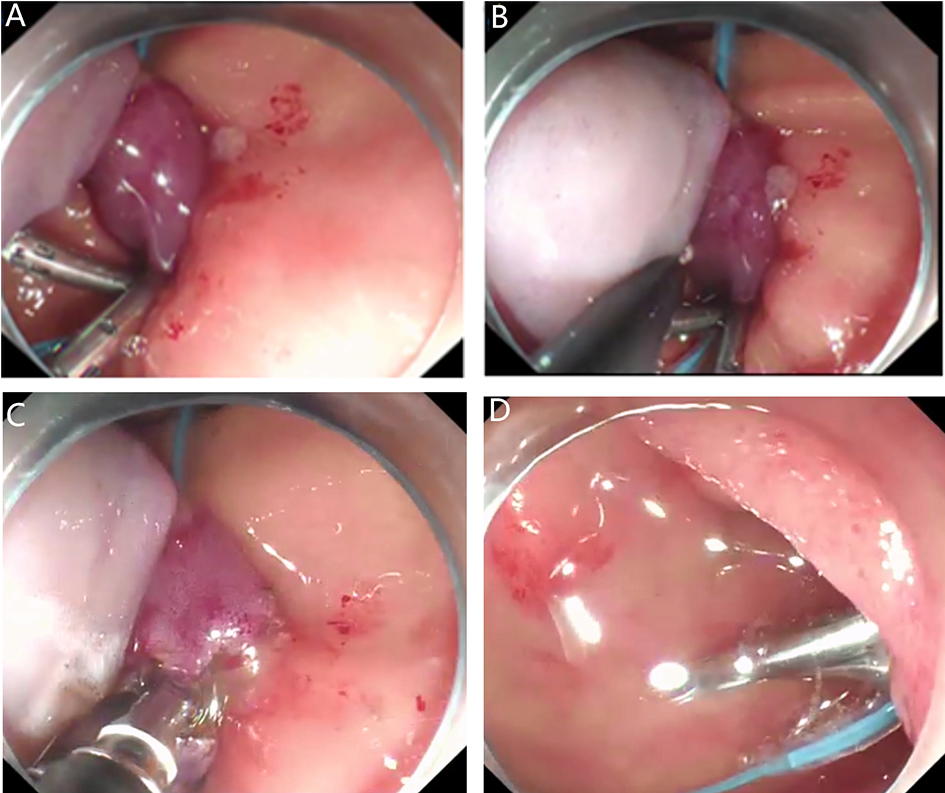
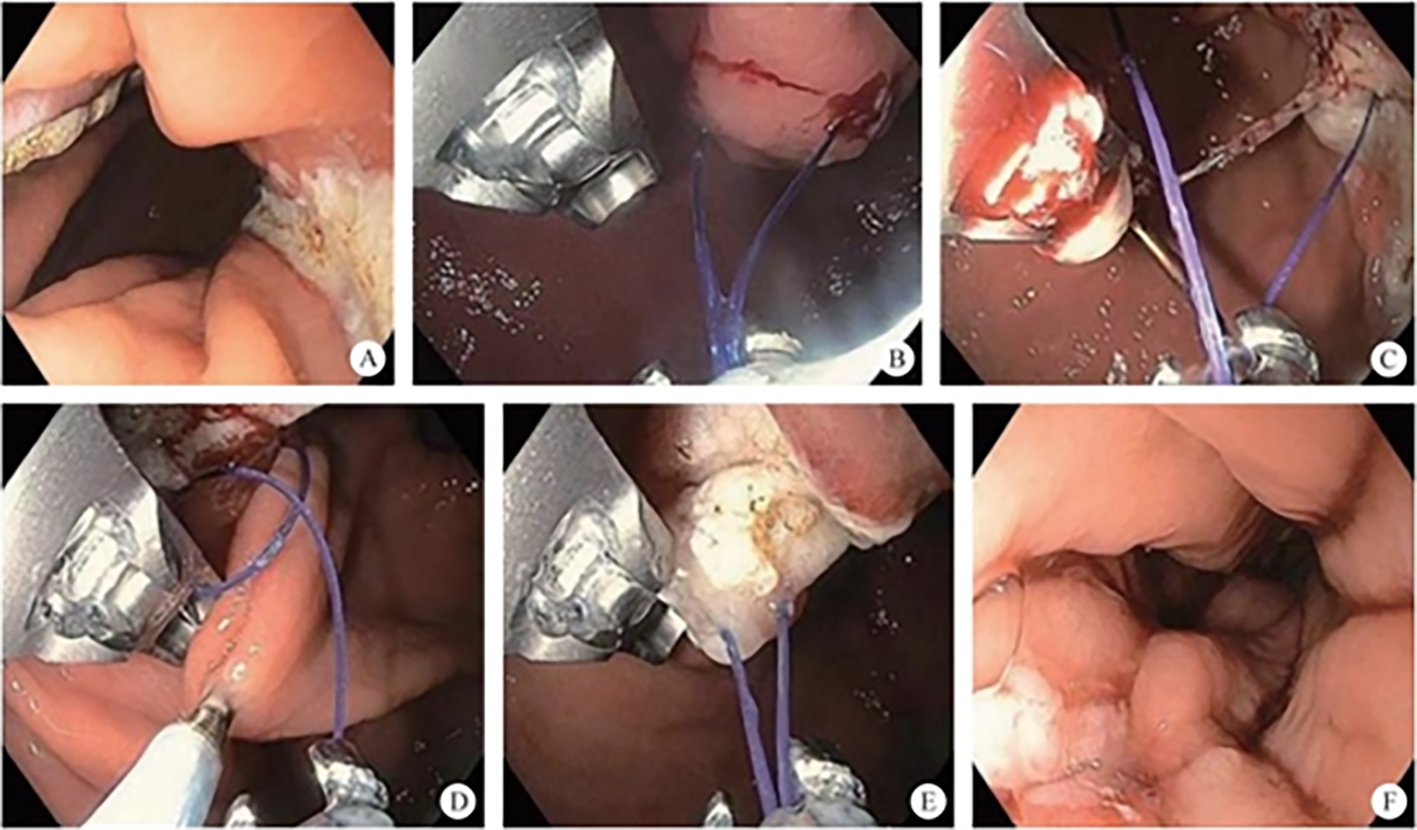
8.5.5 Clip Band Ligation Anti-Reflux Therapy for Gastroesophageal Reflux Disease
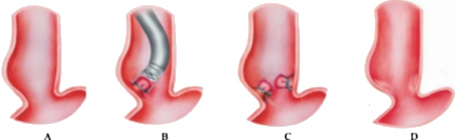

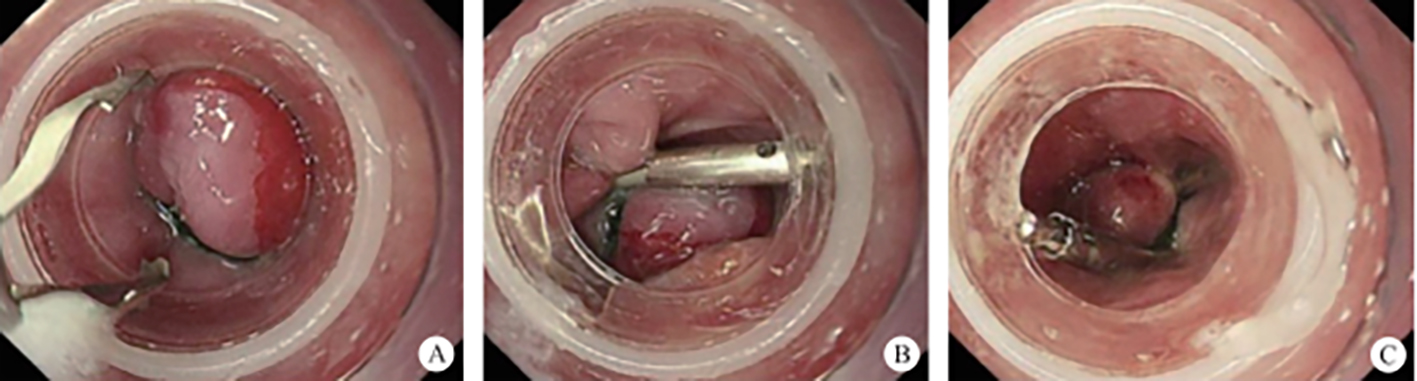
After full preoperative evaluation and having signed the surgery informed consent form, the patient has undergone C-BLART therapy (Refer to video 8.8, Super minimally invasive cardiac constriction for gastroesophageal reflux disease: Cardiac orifice narrowing via Band Ligation and Additional Reinforcement Techniques (See online resources)).
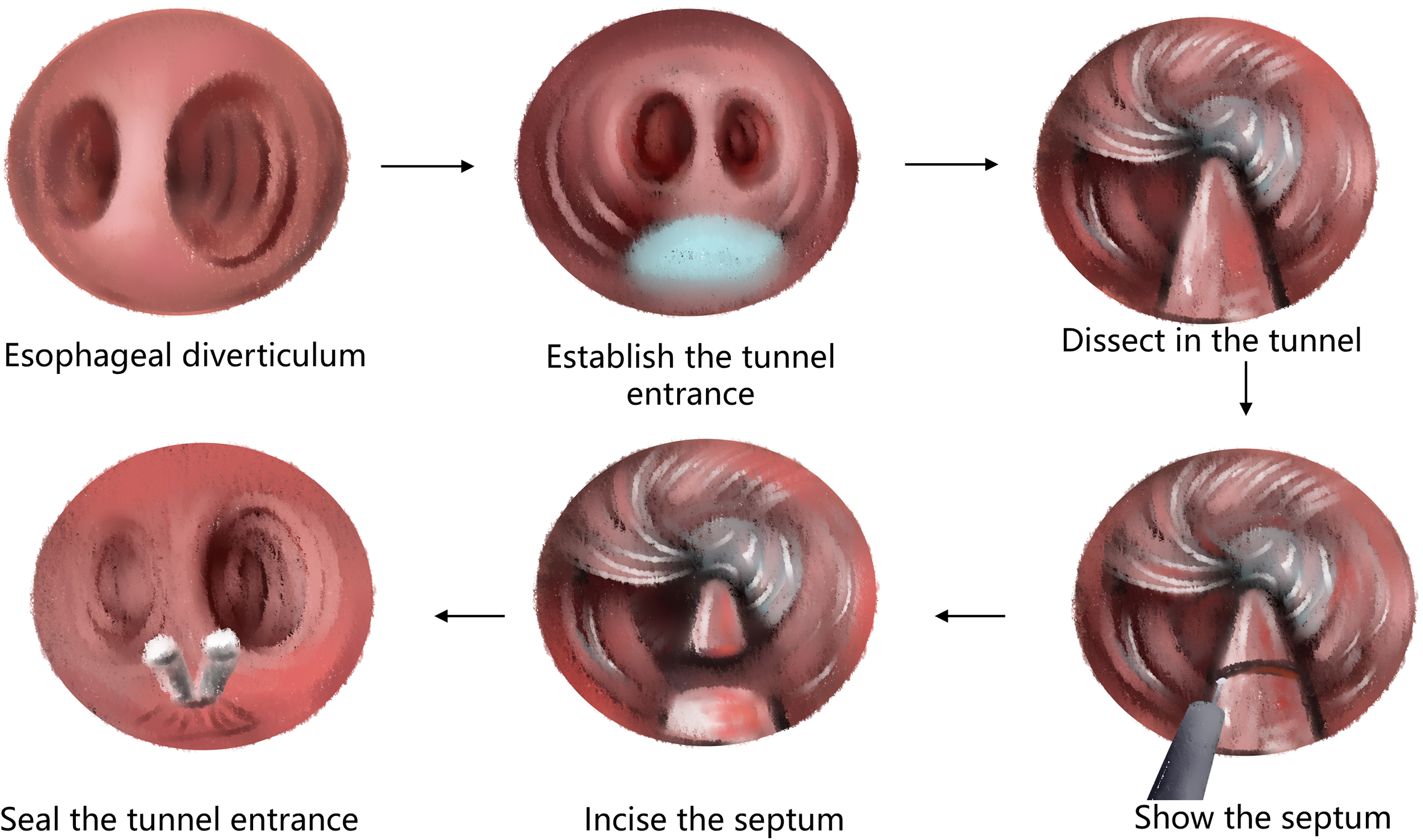
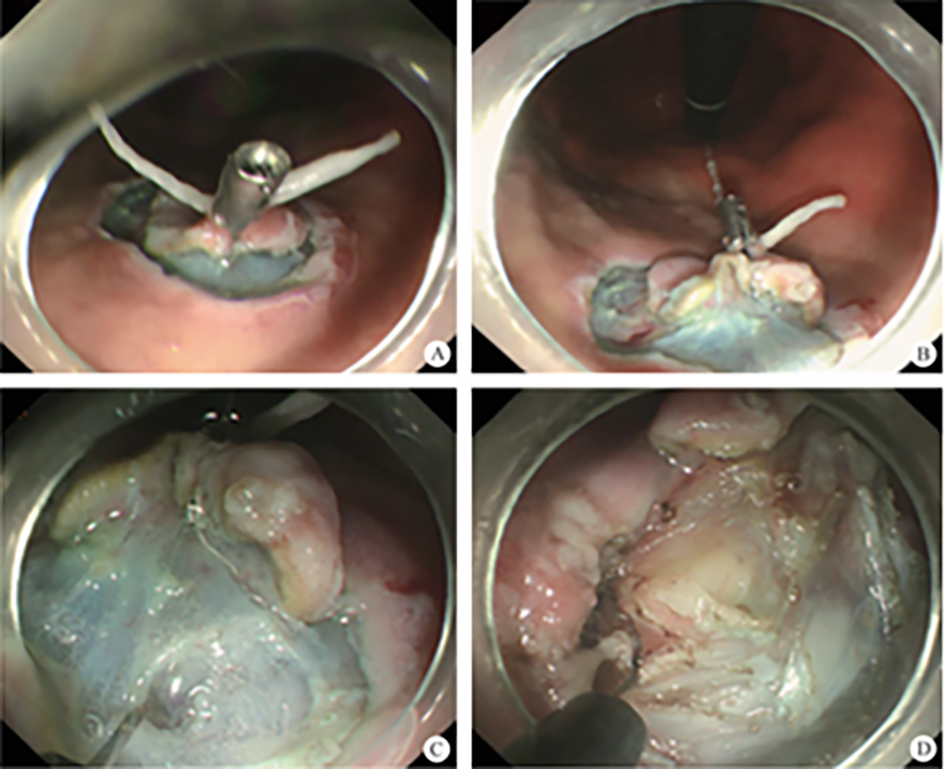
8.6 Super Minimally Invasive Peroral Myotomy of Esophageal Diverticula
8.6.1 Diagnosis of Esophageal Diverticula
8.6.2 STESD’s Indication and Contraindication
8.6.3 Preoperative Preparation
After full preoperative evaluation, improving nutrition state and signing the surgery informed consent form, the patient was performed peroral endoscopic super minimally invasive myotomy for Zenker’s diverticulum (Refer to video 8.9, Per-tunnel super minimally invasive myotomy for esophageal Zenker’s diverticulum (See online resources)).
After full preoperative evaluation and signing the surgery informed consent form, the patient was performed achalasia POEM surgery and STESD surgical therapy for giant esophageal diverticulum (Refer to video 8.10, Per-tunnel super minimally invasive myotomy for lower esophageal diverticulum (See online resources)).
8.7 Super Minimally Myotomy for Achalasia
8.7.1 Introduction
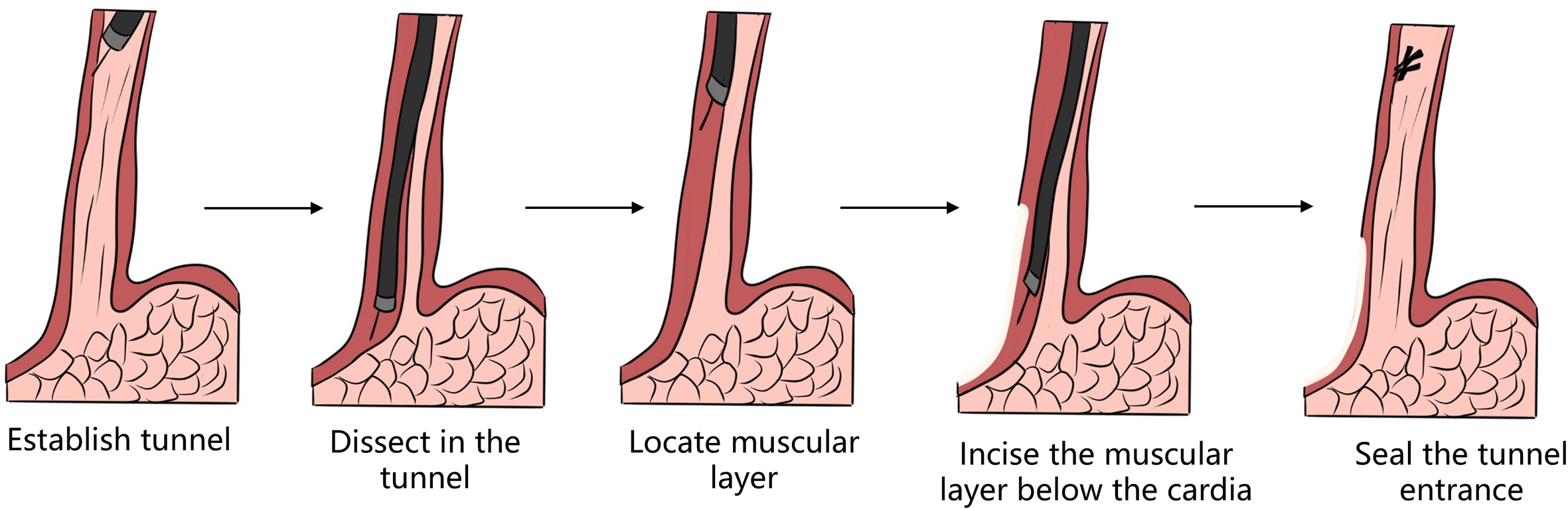
8.7.2 Per-Tunnel Super Minimally Myotomy for Achalasia
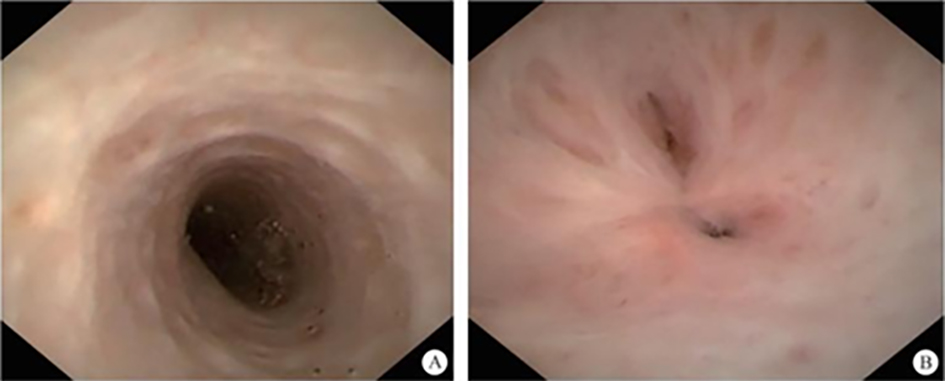
| Typing | Endoscopic manifestation |
| Type I | Mild dilation of lumen, smooth tube wall without winding |
| II | Dilated lumen, with ring or crescent structure after full inflation |
| II a | A thin ring, without crescent shaped structure |
| II b | With crescent structure, not exceeding 1/3 of the lumen |
| II c | With crescent structure, exceeding 1/3 of the lumen |
| III | Obvious lumen dilation, with diverticular structure formation |
| III 1 | Diverticular structure on the left |
| III r | Diverticular structure on right |
| III lr | Diverticular structure found both on the left and on the right |
Refer to video 8.11, Per-tunnel super minimally myotomy for achalasia-1 (See online resources).
After full preoperative evaluation, improving nutrition condition and signing the surgery informed consent form, the patient was performed achalasia POEM surgery (Refer to video 8.12, Per-tunnel super minimally myotomy for achalasia-2 (See online resources)).
References
Chapter 9 Super Minimally Invasive Surgery of Gastric Diseases
9.1 Super Minimally Invasive Surgery for Early Gastric Cancer
9.1.1 Overview
| Serial no. | Super minimally invasive surgery (SMIS) | Technical method | Previous nomenclature |
| 1 | Peroral SMIS for early gastric cancer | Non-full-thickness resection | Endoscopic submucosal dissection (ESD), traction-assisted ESD, transparent cap-assisted endoscopic mucosal resection (EMR) |
| 2 | Peroral SMIS for early gastric cancer | Full-thickness resection | Endoscopic full-thickness resection (EFTR), traction-assisted EFTR |
| 3 | Per-tunnel SMIS for early gastric cancer | Non-full-thickness resection | Submucosal tunneling endoscopic resection (STER), traction-assisted ESD |
| 4 | Per-multiple-cavity SMIS for early gastric cancer | Multi-cavity minimally invasive resection | Multiscope-assisted therapy |
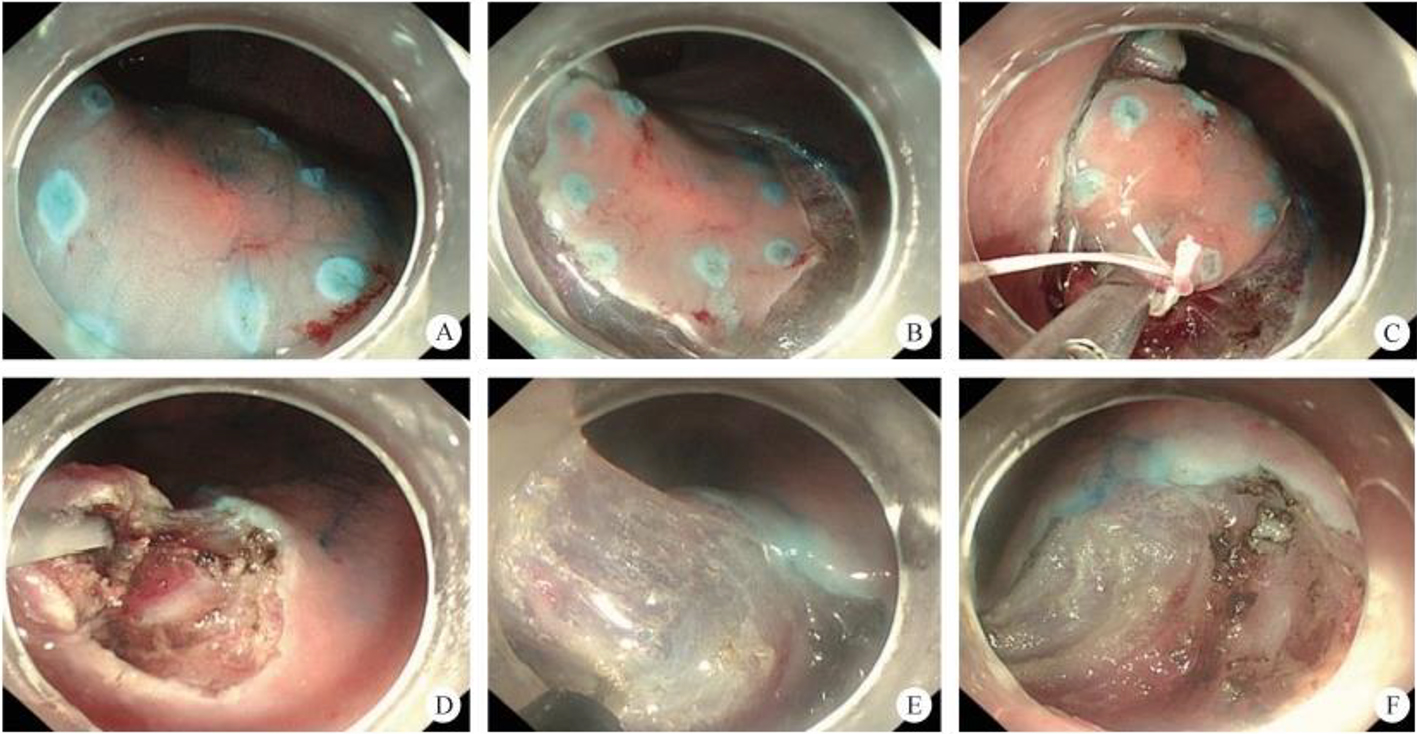
9.1.2 Peroral Super Minimally Invasive Surgery by Non-Full-Thickness Resection for Early Gastric Cancer
Refer to video 9.1, Peroral super minimally invasive non-full-thickness resection for early cancer at the gastric cardia and fundus (See online resources).
Refer to video 9.2, Peroral super minimally invasive non-full-thickness resection for early cancer of the gastric body (See online resources).
Refer to video 9.3, Super minimally invasive non-full-thickness resection for early cancer of the gastric antrum (See online resources).
Refer to video 9.4, Super minimally invasive non-full-thickness resection for early gastric angular cancer (See online resources).
After thorough preoperative evaluation, nutritional status improvement, and obtaining informed surgical consent, the patient underwent an ESD-assisted dental floss traction procedure. Refer to video 9.5, Super minimally invasive non-full-thickness resection for early cancer of the gastric antrum (See online resources).
9.1.3 Super Minimally Invasive Full-Thickness Resection for Early Gastric Cancer
Refer to video 9.6, Super minimally invasive full-thickness resection for early gastric cancer of the gastric body (See online resources).
9.1.4 Early Gastric Cancer: Super Minimally Invasive Resection via the Tunnel Technique
9.1.5 Early Gastric Cancer Treated with Multi-Channel Super Minimally Invasive Resection
9.2 Super Minimally Invasive Surgery for Gastric Low-Grade Intraepithelial Neoplasia
9.2.1 Overview
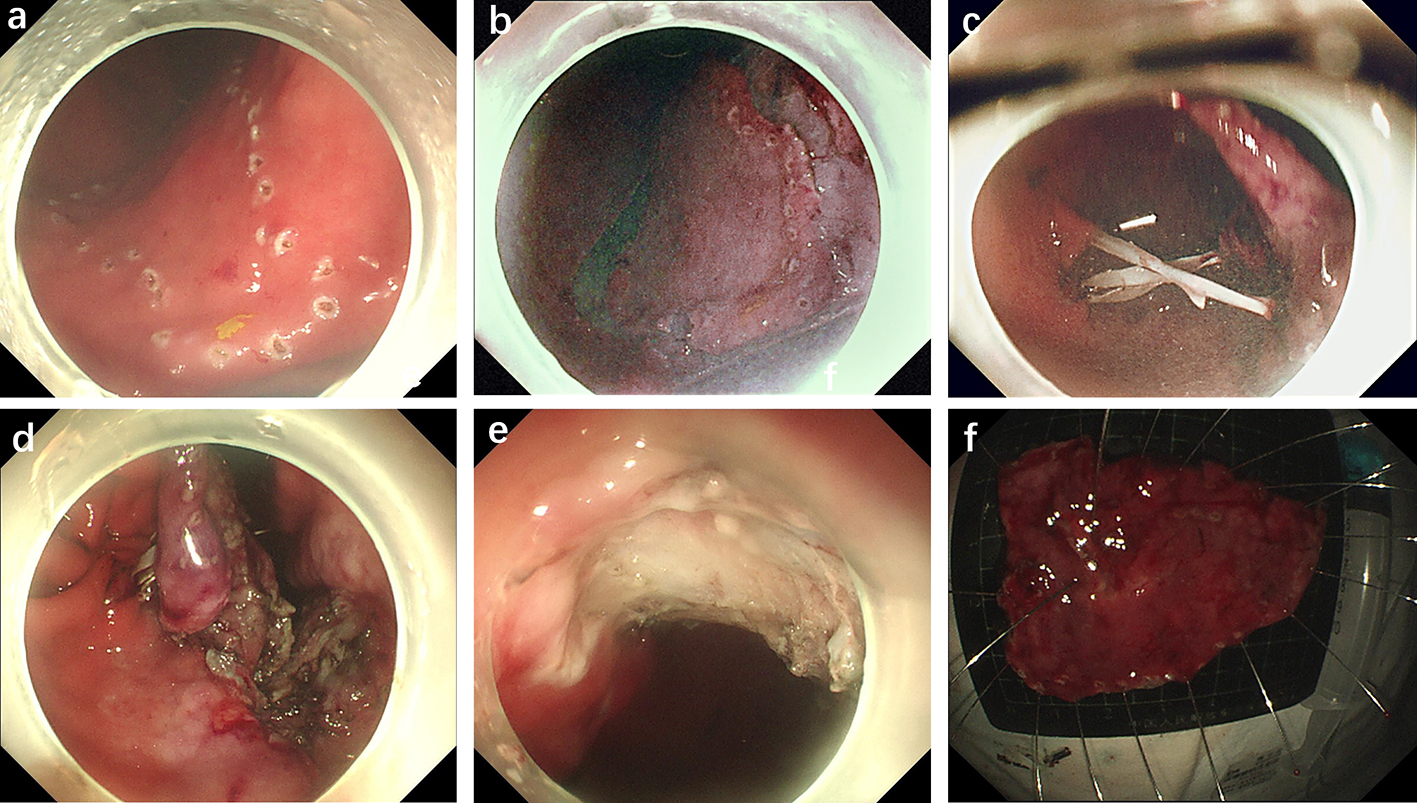
9.2.2 Low-Grade Intraepithelial Neoplasia of the Stomach: Peroral Super Minimally Invasive Radiofrequency Ablation
Refer to video 9.7, Super minimally invasive radiofrequency ablation for gastric low-grade intraepithelial neoplasia (See online resources).
9.2.3 Low-Grade Gastric Intraepithelial Neoplasia: Super Minimally Invasive Argon Plasma Coagulation
9.2.4 Low-Grade Gastric Intraepithelial Neoplasia: Super Minimally Invasive Holmium Laser Therapy
9.3 Super Minimally Invasive Resection of Gastric Subepithelial Tumors
9.3.1 Overview
| No. | SMIS technique | Technical method | Historical nomenclature |
| 1 | Traction-assisted endoscopic submucosal dissection | Peroral super minimally invasive resection | Endoscopic submucosal dissection (ESD)Traction-assisted endoscopic submucosal dissectionCap-assisted endoscopic mucosal resection (EMR)Endoscopic mucosal resection (EMR)Endoscopic submucosal tumor excavation |
| 2 | Peroral super minimally invasive resection of gastric subepithelial tumors | Super minimally invasive full-thickness resection | Endoscopic full-thickness resection (EFTR)Traction-assisted endoscopic full-thickness resection |
| 3 | Per-tunnel super minimally invasive resection of gastric subepithelial tumors | Super minimally invasive non-full-thickness resection | Endoscopic submucosal tunneling dissectionTraction-assisted endoscopic submucosal dissection |
| 4 | Per-multiple-cavity super minimally invasive resection of gastric subepithelial tumors | Super minimally invasive multi-cavity resection | Combined multiscope therapy |
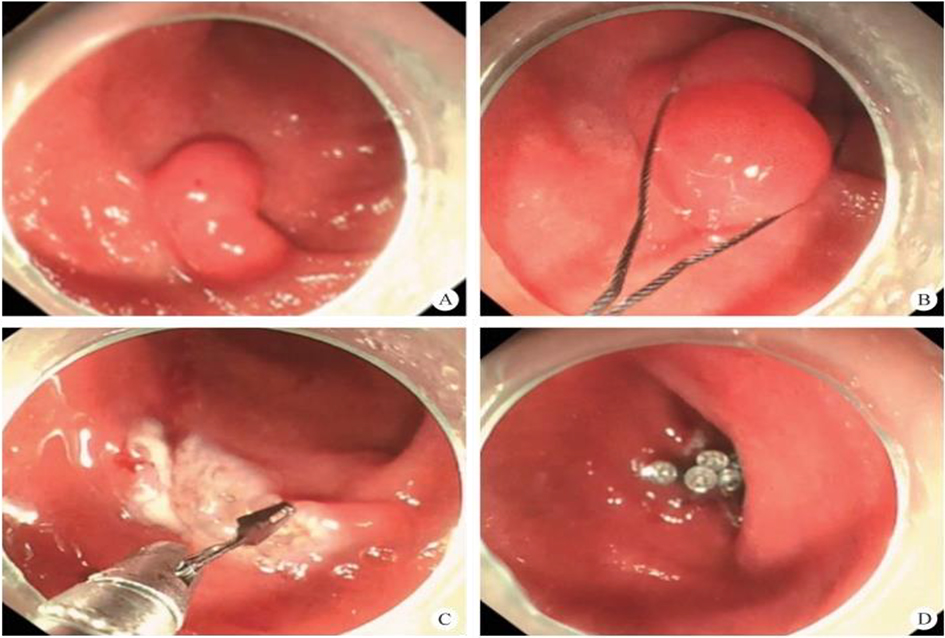
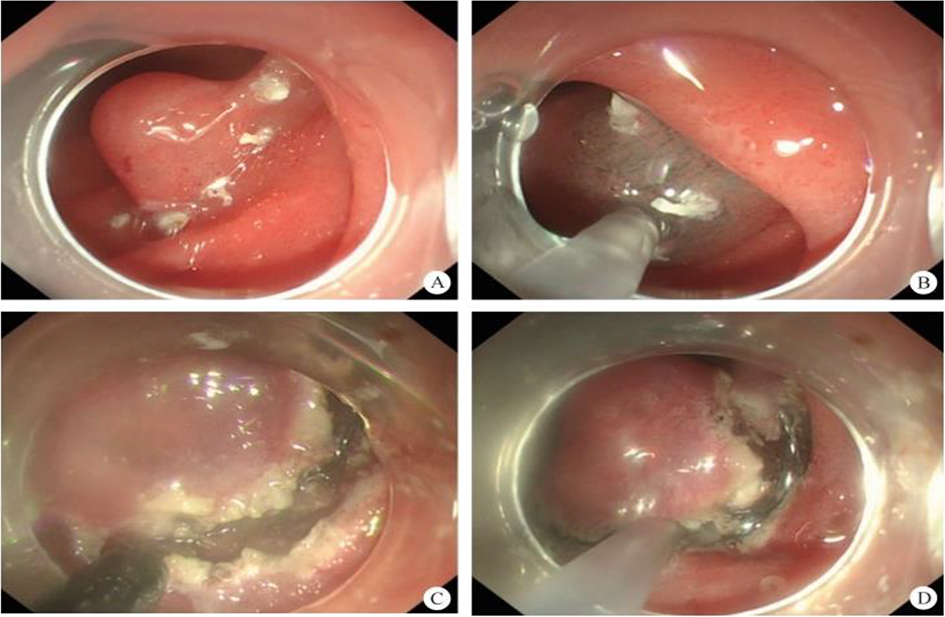
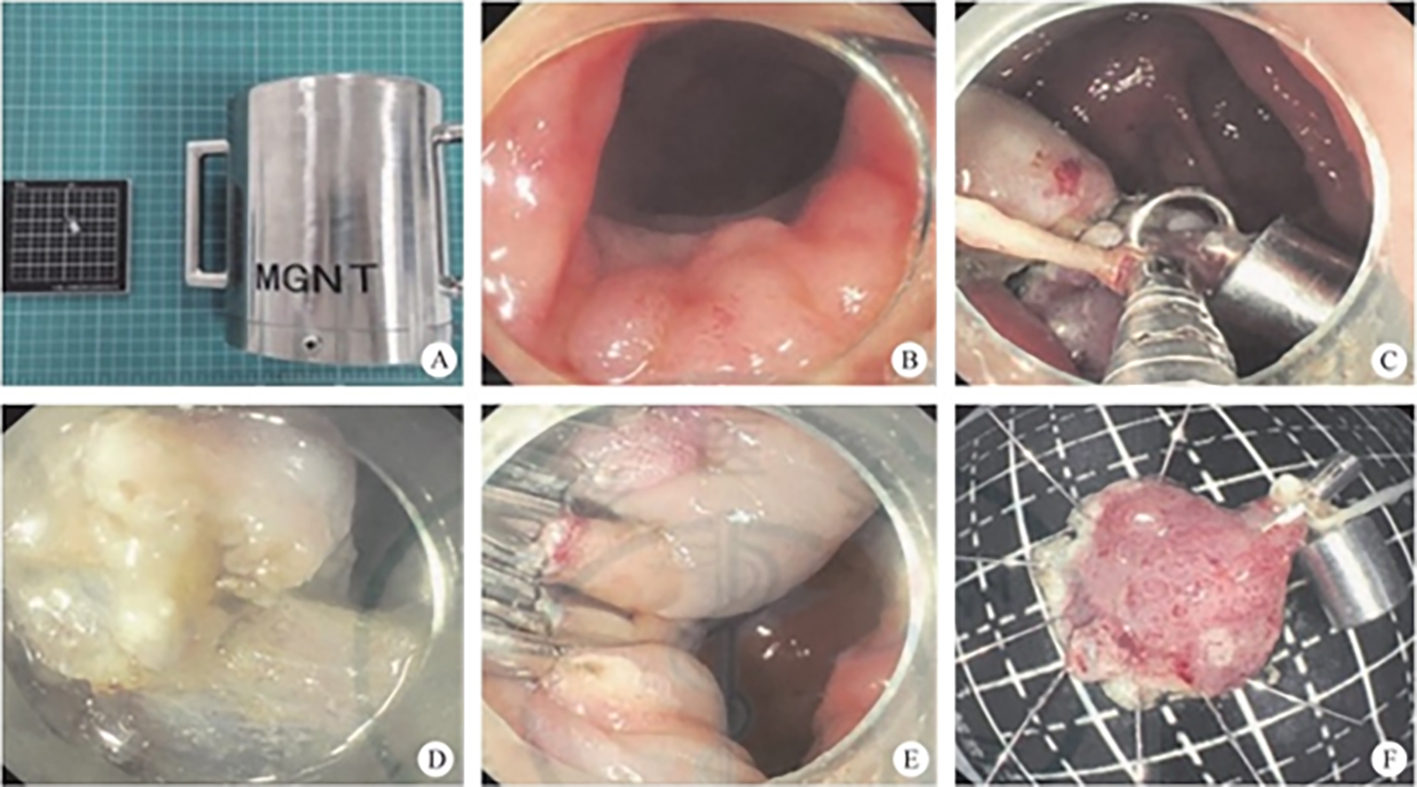
9.3.2 Super Minimally Invasive Resection of Gastric Subepithelial Tumors
After thorough preoperative evaluation, nutritional status optimization, and obtaining informed consent for surgery, the patient underwent a super minimally invasive peroral resection procedure. Refer to video 9.9, Super minimally invasive peroral resection of subepithelial tumor of the cardia) (See online resources).
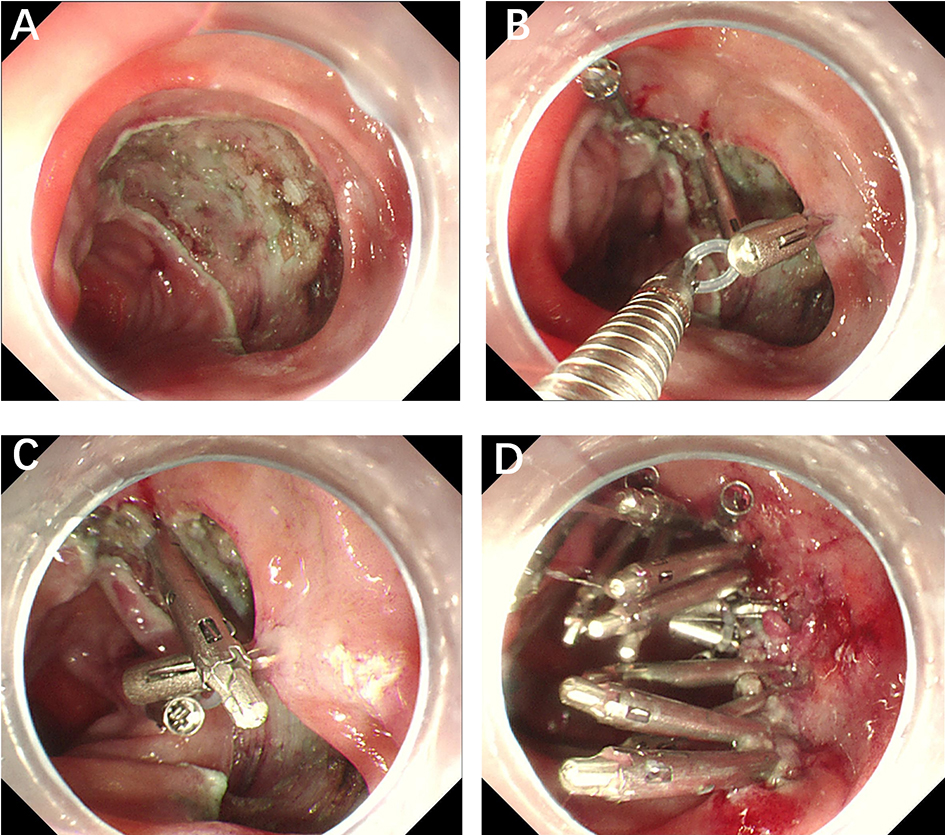
9.3.3 Peroral Super Minimally Invasive Full-Thickness Resection of Gastric Subepithelial Tumors
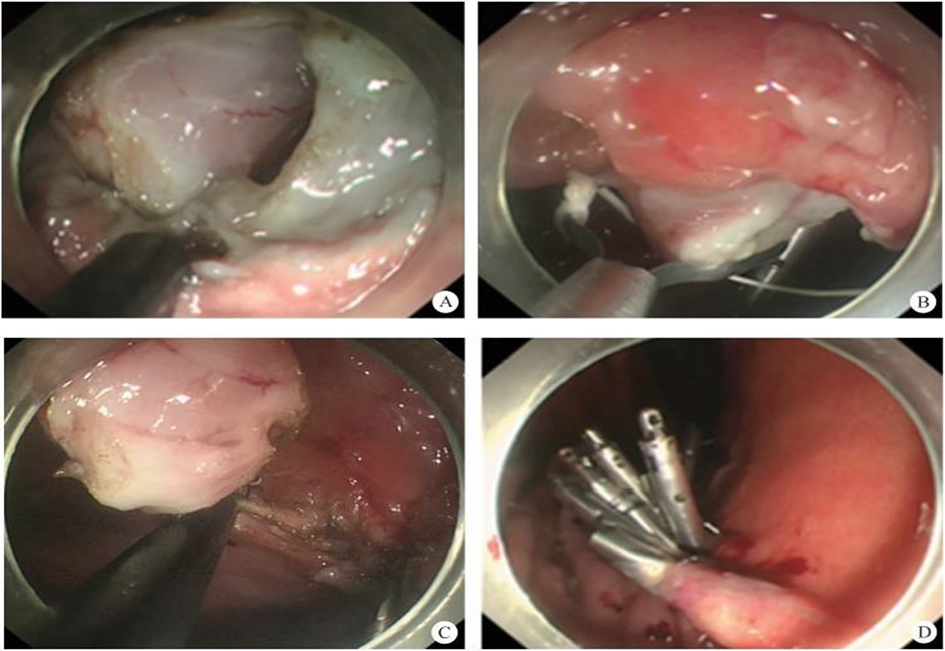
After thorough preoperative evaluation, nutritional optimization, and informed consent, the patient underwent peroral Super minimally invasive resection. Refer to video 9.10, Peroral super minimally invasive full-thickness resection of a subepithelial tumor in the gastric body (See online resources).
Refer to video 9.11, Peroral super minimally invasive full-thickness resection of a tumor in the lesser sac of the gastric fundus (See online resources).
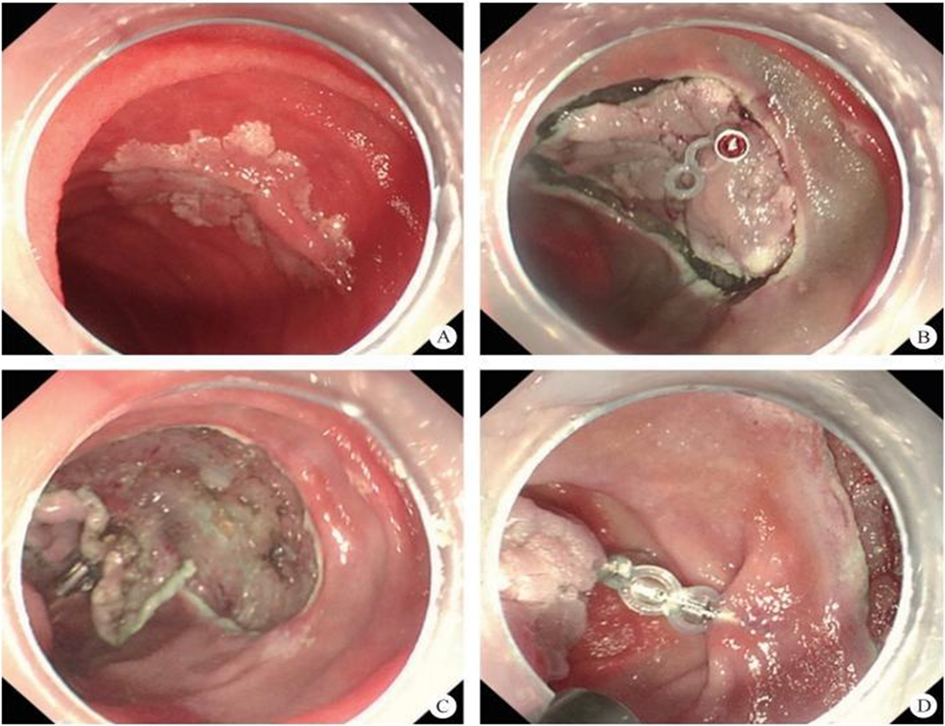
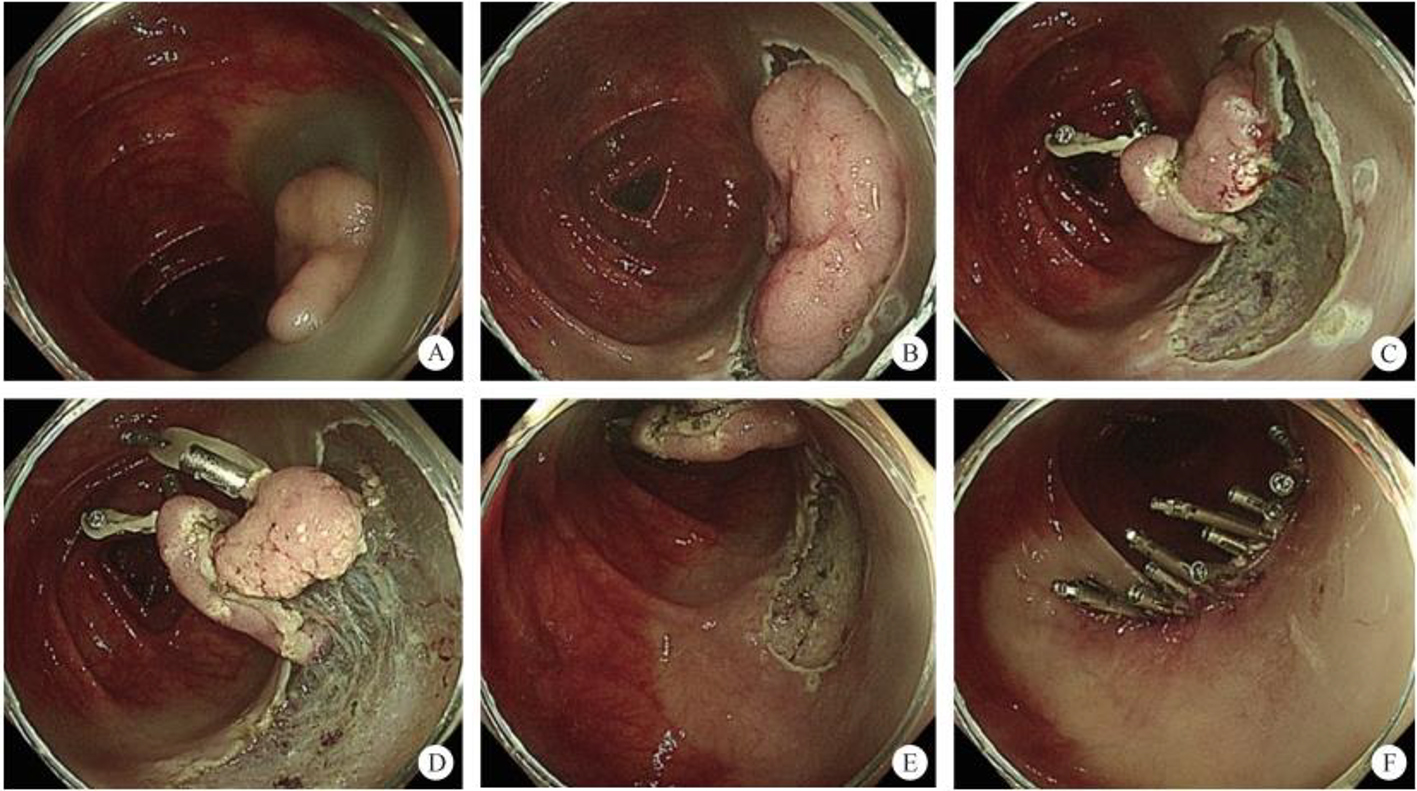
9.3.4 Peroral Super Minimally Invasive Non-Full-Thickness Resection of Gastric Subepithelial Tumors
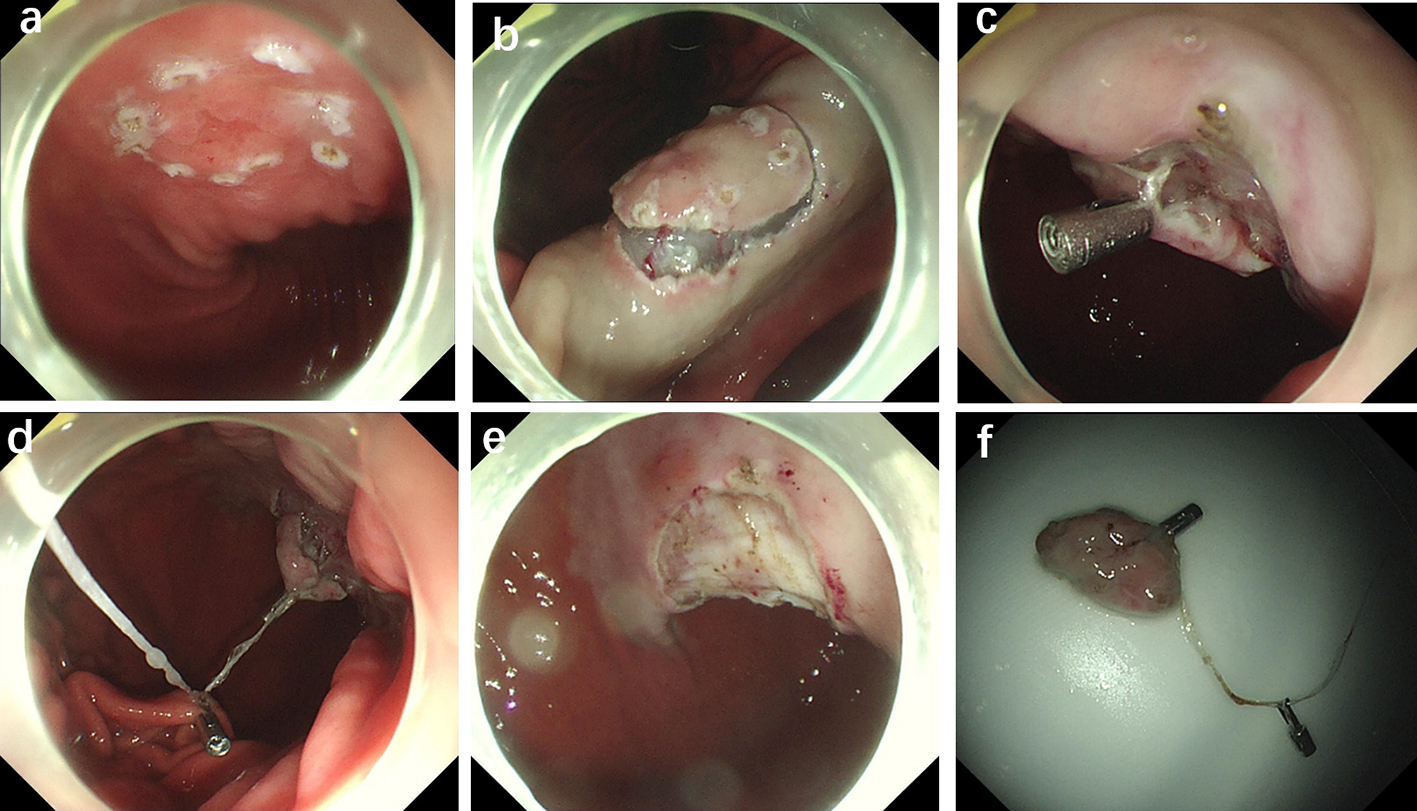
Refer to video 9.12, Peroral super minimally invasive non-full-thickness resection of multiple gastric neuroendocrine tumors (See online resources).
9.3.5 Trans-Multi-Cavitary Super Minimally Invasive Resection of Gastric Subepithelial Tumors
9.4 Super Minimally Invasive Surgery for Gastroparesis
9.4.1 Overview
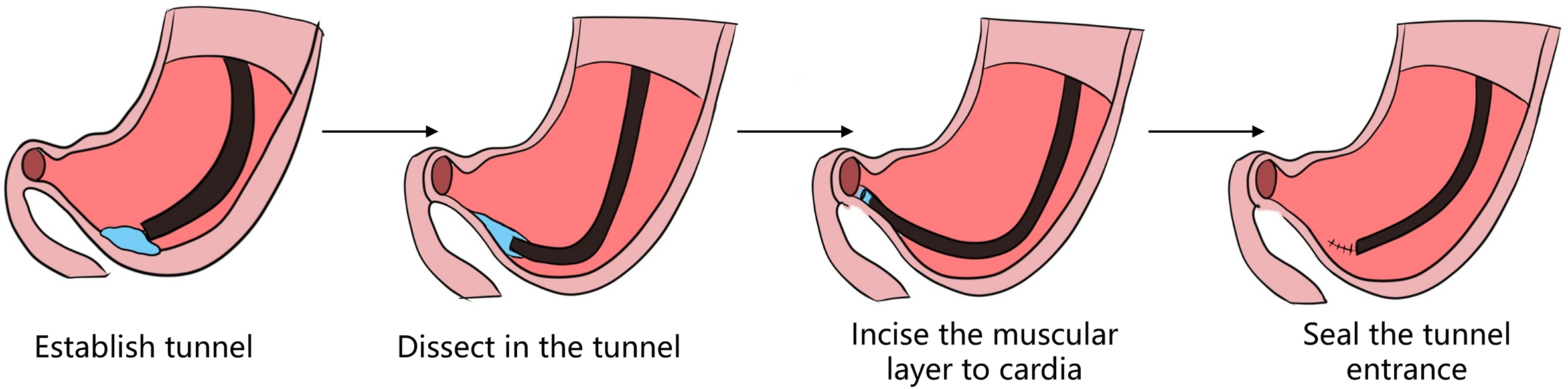
9.4.2 Super Minimally Invasive Tunnel Myotomy for Gastroparesis
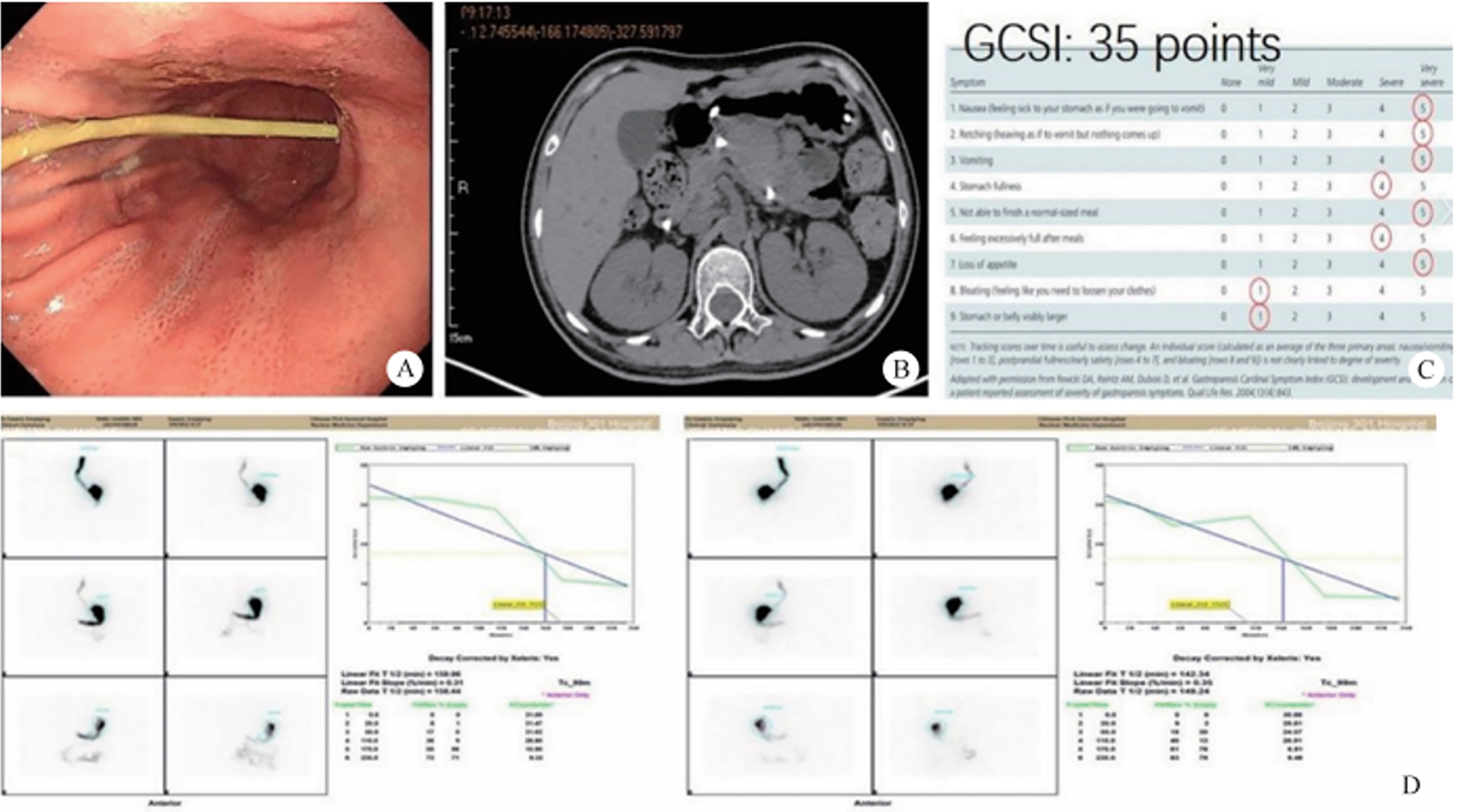
Refer to video 9.13, Super minimally invasive peroral endoscopic myotomy for gastroparesis (See online resources).
9.4.3 Gastric Peroral Super Minimally Invasive Botulinum Toxin Injection (BoNT)
9.4.4 Peroral Super Minimally Invasive Pyloric Stenting for Gastroparesis

References
Chapter 10 Super Minimally Invasive Therapies for Duodenal Diseases
10.1 Peroral Super Minimally Invasive Resection for Early Duodenal Cancer
After comprehensive preoperative evaluation, nutritional optimization, and informed consent, the patient underwent a peroral super minimally invasive resection of the duodenal LST (Refer to video 10.1, Peroral super minimally invasive non-full-thickness resection of duodenal LST (See online resources)).
10.2 Peroral Super Minimally Invasive Resection of Duodenal Papillary Adenomas
10.2.1 Overview
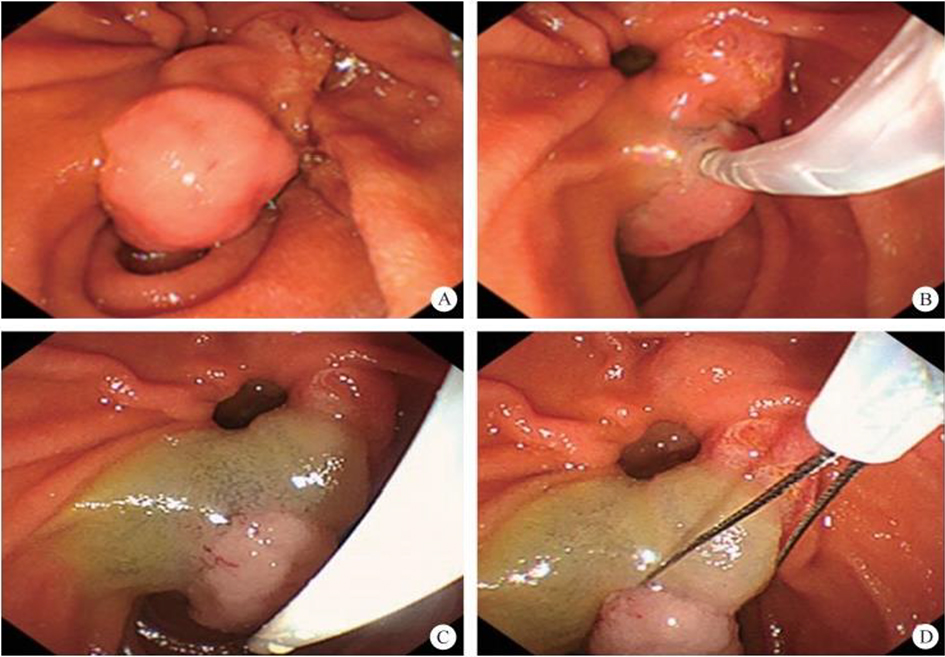
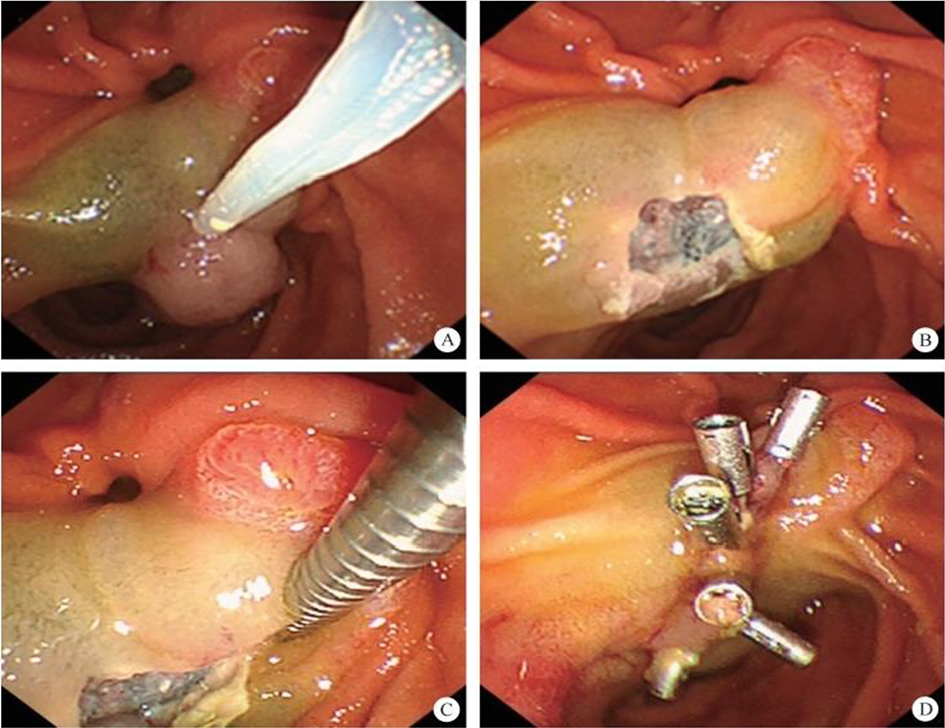
(n) The excised specimen was sent for pathological analysis. Refer to video 10.2, Peroral super minimally invasive resection of a duodenal ampullary adenoma (See online resources).
10.3 Peroral Super Minimally Invasive Resection of Subepithelial Duodenal Tumors
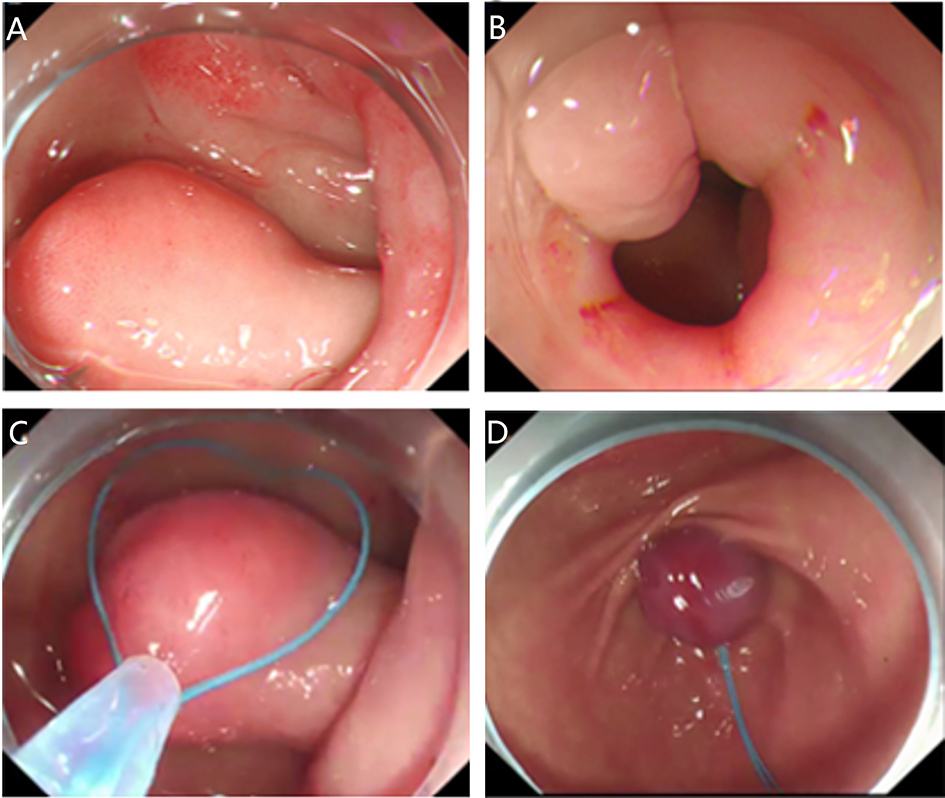
Following thorough preoperative evaluation, nutritional improvement, and signing of the informed surgical consent form, the patient underwent a peroral super minimally invasive resection of a duodenal subepithelial tumor (Refer to video 10.3, Peroral super minimally invasive resection of a subepithelial tumor in the descending duodenum-1 (See online resources)).
Following thorough preoperative evaluation, nutritional improvement, and signing of informed surgical consent form, the patient underwent a peroral super minimally invasive resection of the duodenal subepithelial tumor (Refer to video 10.4, Peroral super minimally invasive resection of a subepithelial tumor in the descending duodenum-2 (See online resources)).
10.4 Peroral Super Minimally Invasive Resection of Duodenal Polyps
10.4.1 Overview
10.4.2 Diagnosis of Duodenal Polyps
10.4.3 Indications and Contraindications
10.4.4 Preoperative Preparation
10.4.5 Surgical Procedure and Techniques
Refer to video 10.5, Peroral super minimally invasive non-full-thickness resection of duodenal adenomas-1 (See online resources).
10.4.6 Hot-Spot Issues and Research Progress in the Consensus
Refer to video 10.6, Peroral super minimally invasive non-full-thickness resection of duodenal polyps-2 (See online resources).
References
Chapter 11 Super Minimally Invasive Surgery for Biliary Diseases
11.1 Choledocholithiasis and Cholangitis – Super Minimally Invasive Surgery
11.1.1 Overview
11.1.2 Endoscopic Super Minimally Invasive Retrieval of Choledocholithiasis

After thorough preoperative assessment and obtaining informed consent for surgery, the patient underwent bile duct stone removal via endoscopic retrograde cholangiopancreatography (ERCP) under direct vision (Refer to video 11.1, Super minimally invasive bile duct stone extraction via duodenal papillary bile duct endoscopy (See online resources)).
11.1.3 Peroral Super Minimally Invasive Papillotomy
11.1.4 Acute Suppurative Cholangitis and Peroral Super Minimally Invasive Drainage
11.2 Super Minimally Invasive Surgery of Biliary Strictures
11.2.1 Overview
11.2.2 Super Minimally Invasive Dilatation for Biliary Stricture at the Duodenal Papilla
11.2.3 Biliary Stricture: Super Minimally Invasive Endoscopic Stent Placement at the Duodenal Papilla
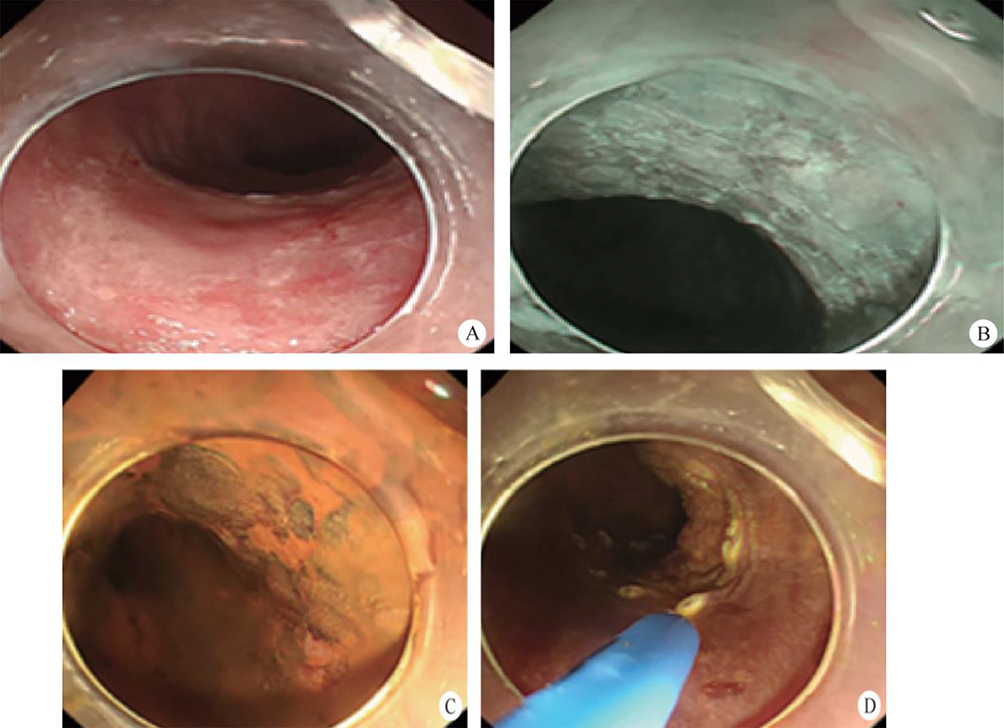
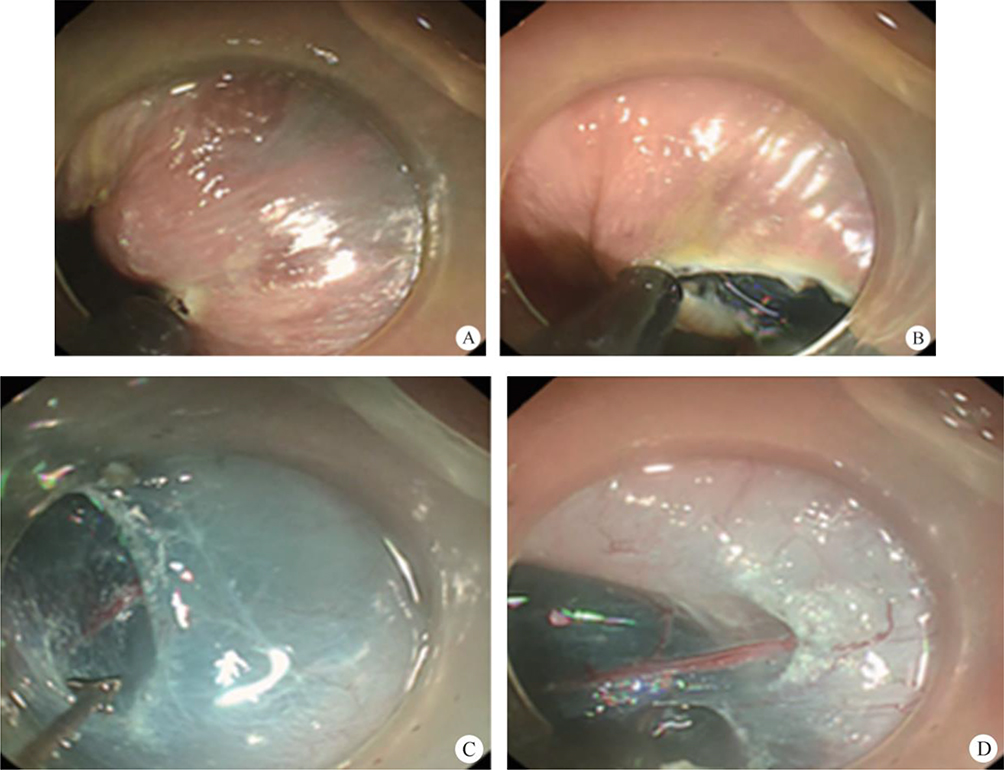
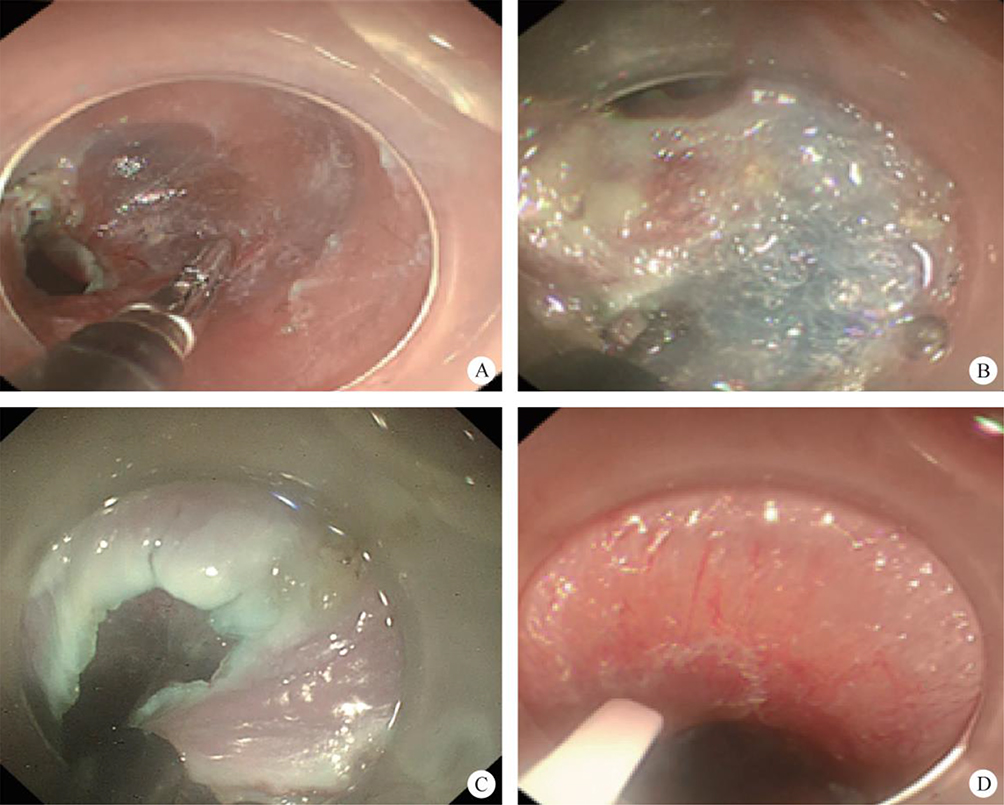
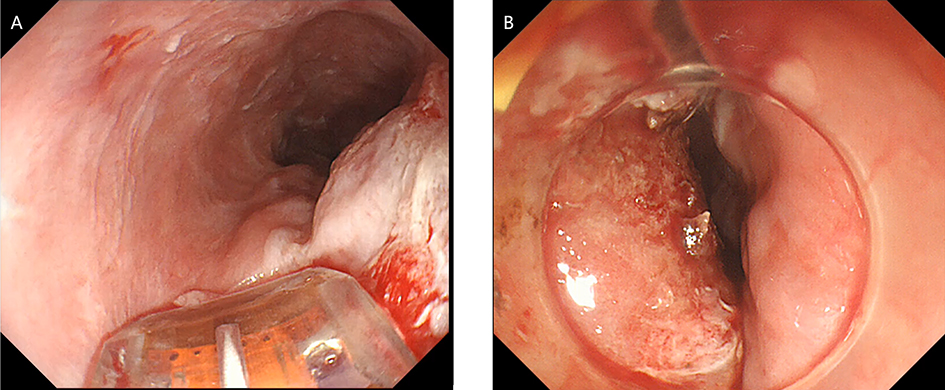
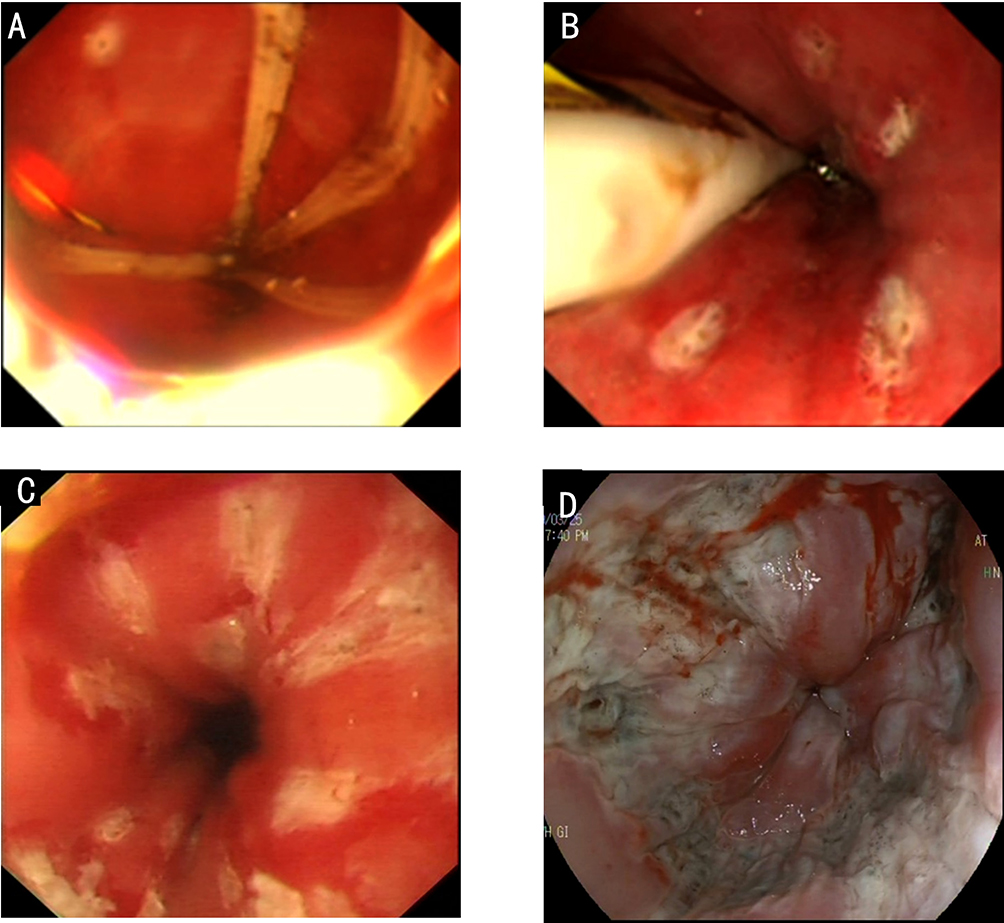
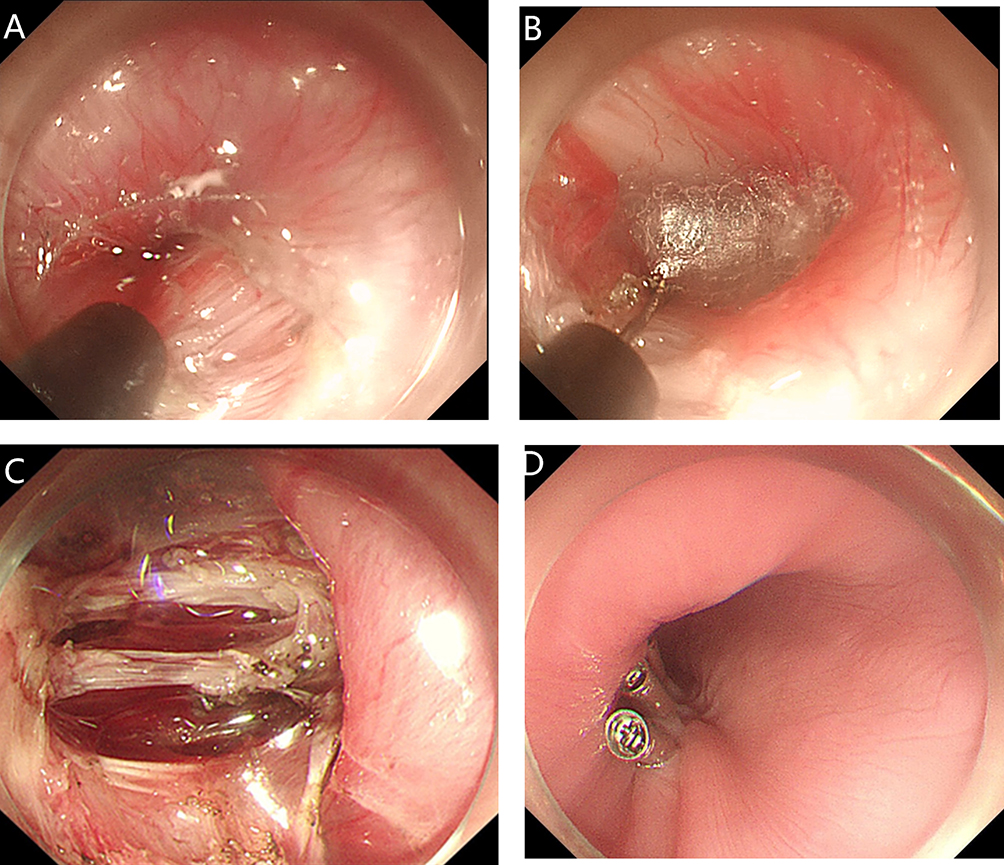
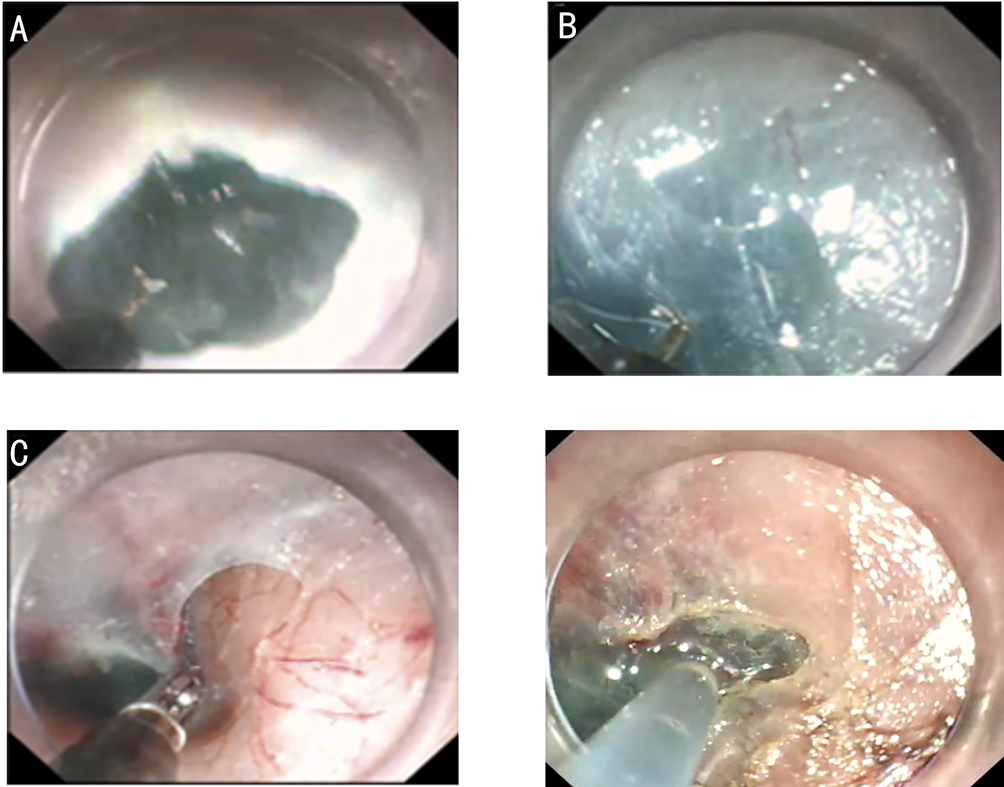
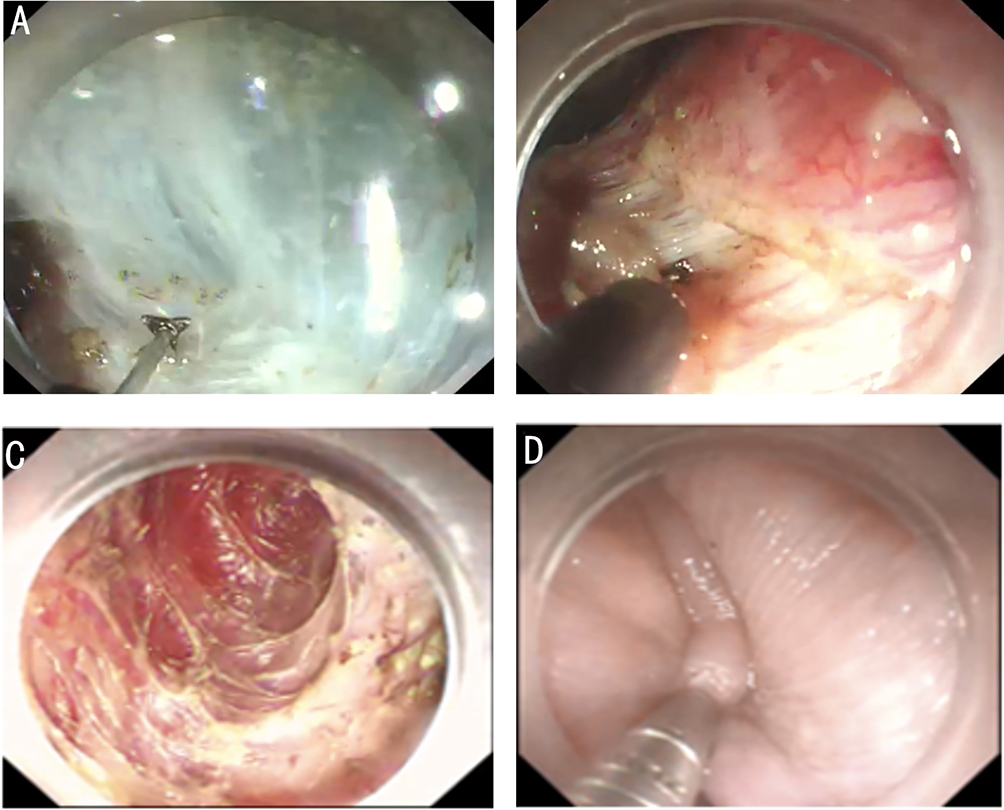
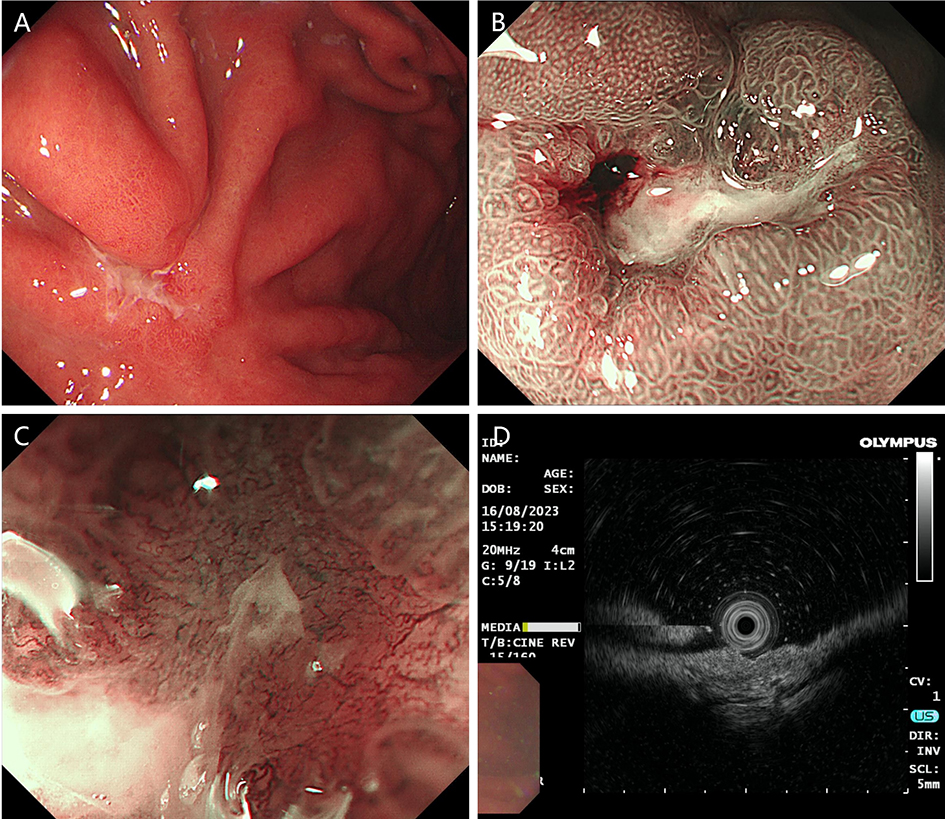
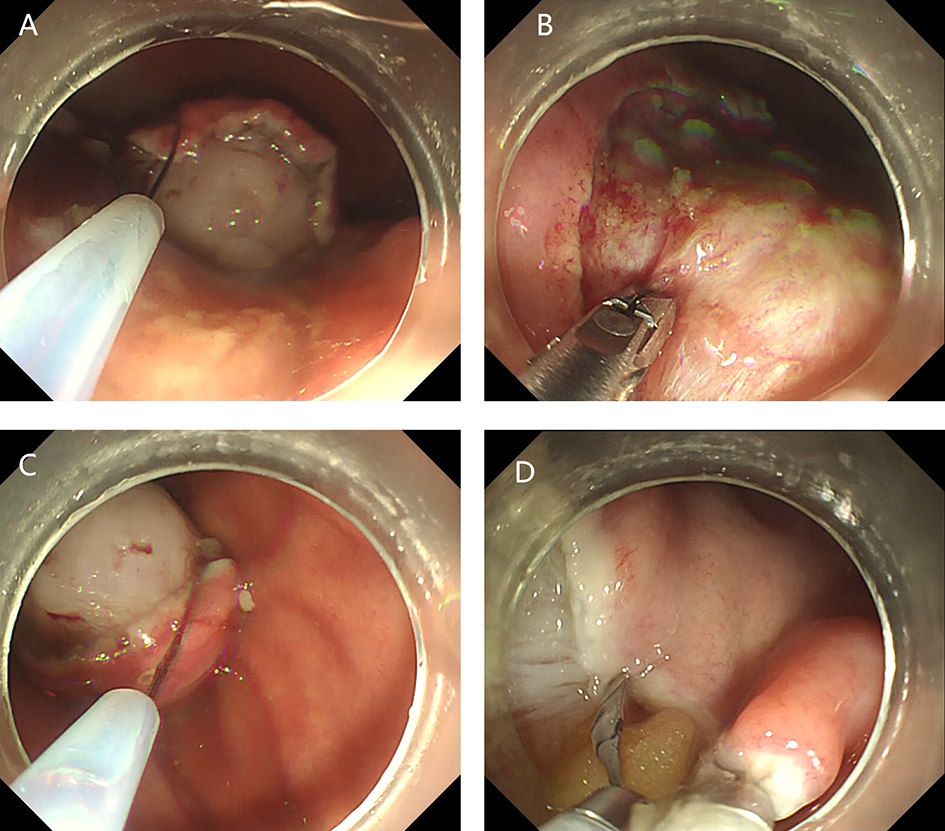
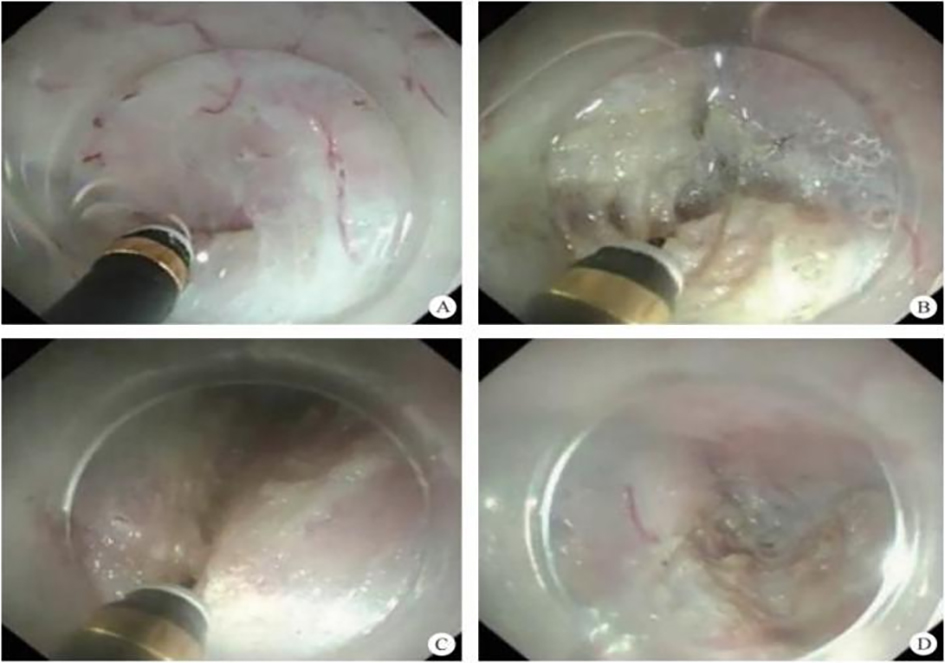
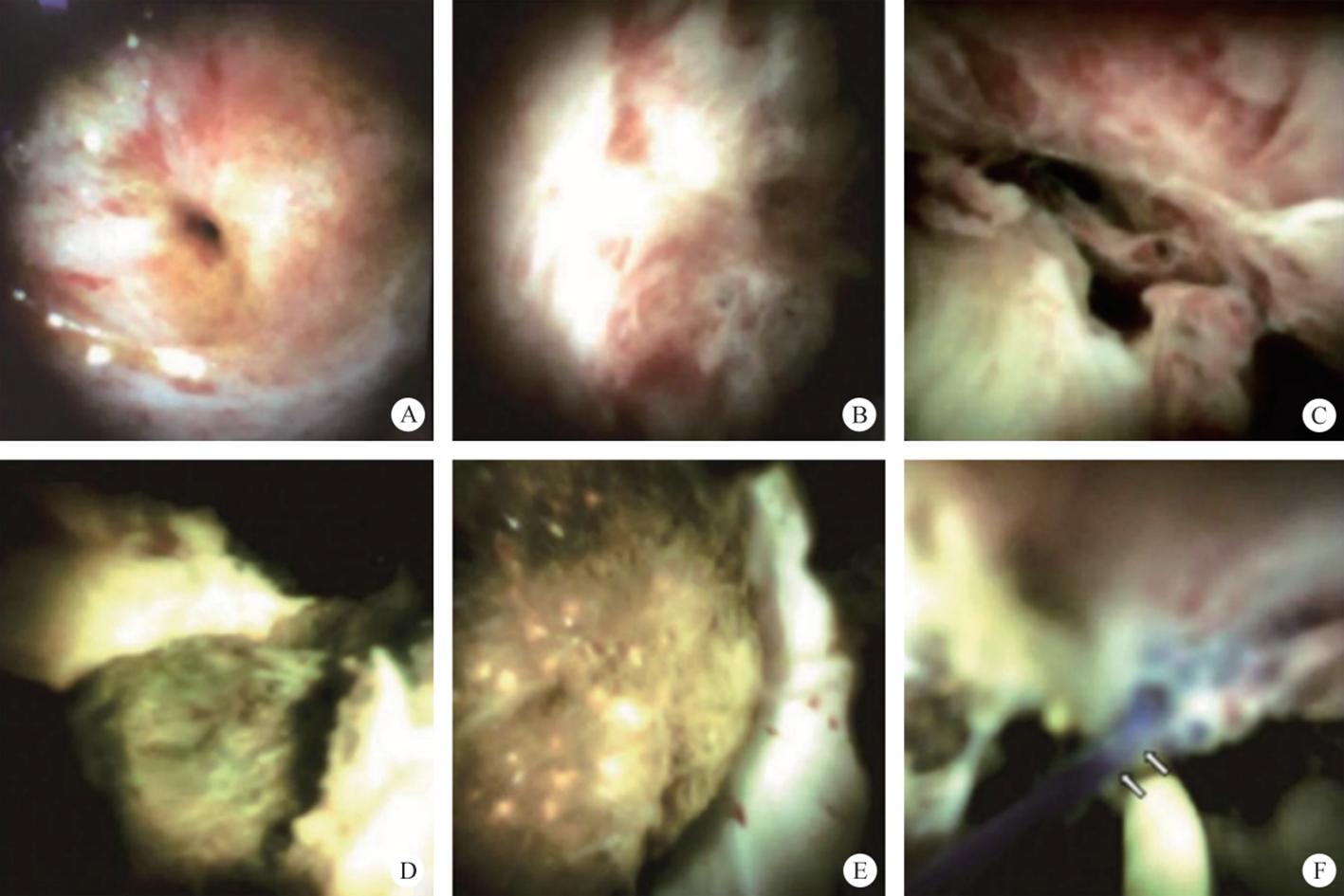
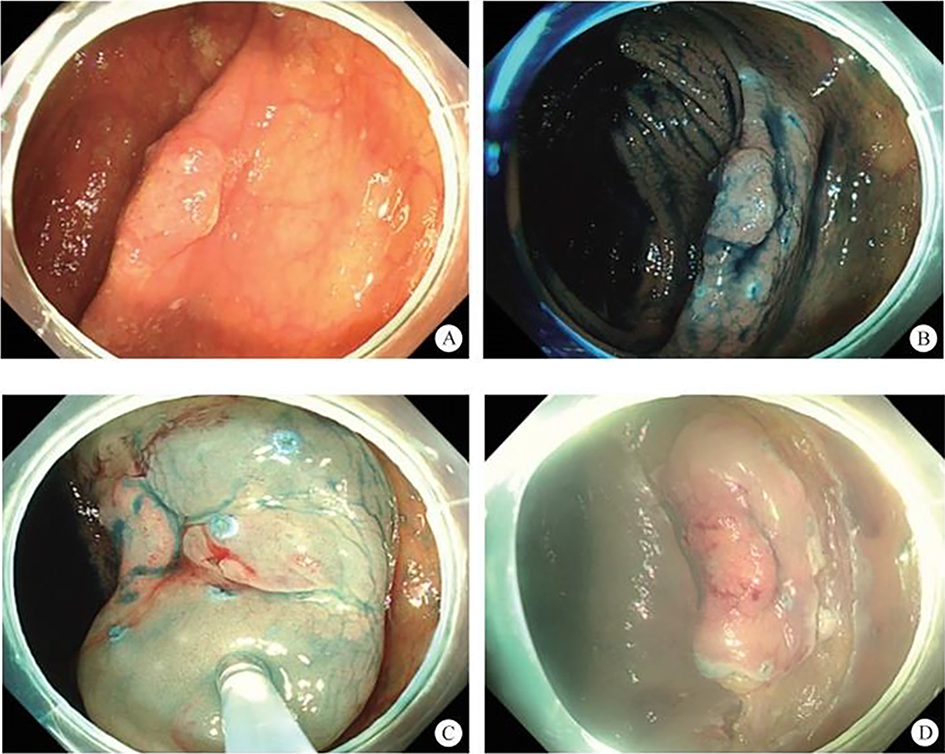
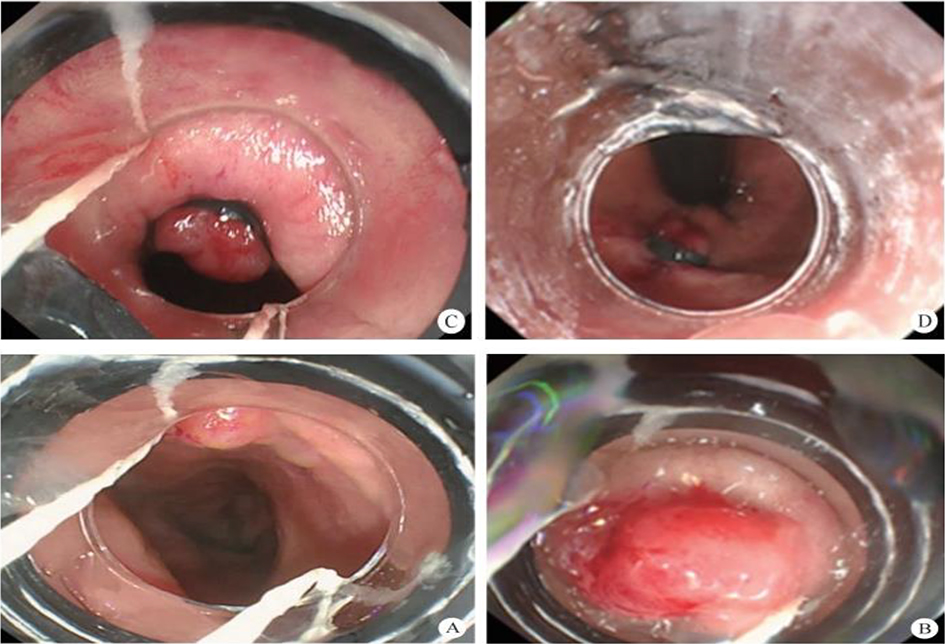
11.2.4 Biliary Stricture: Diagnosis and Treatment with Peroral Cholangiopancreatoscopy (POC) Under Direct Visualization
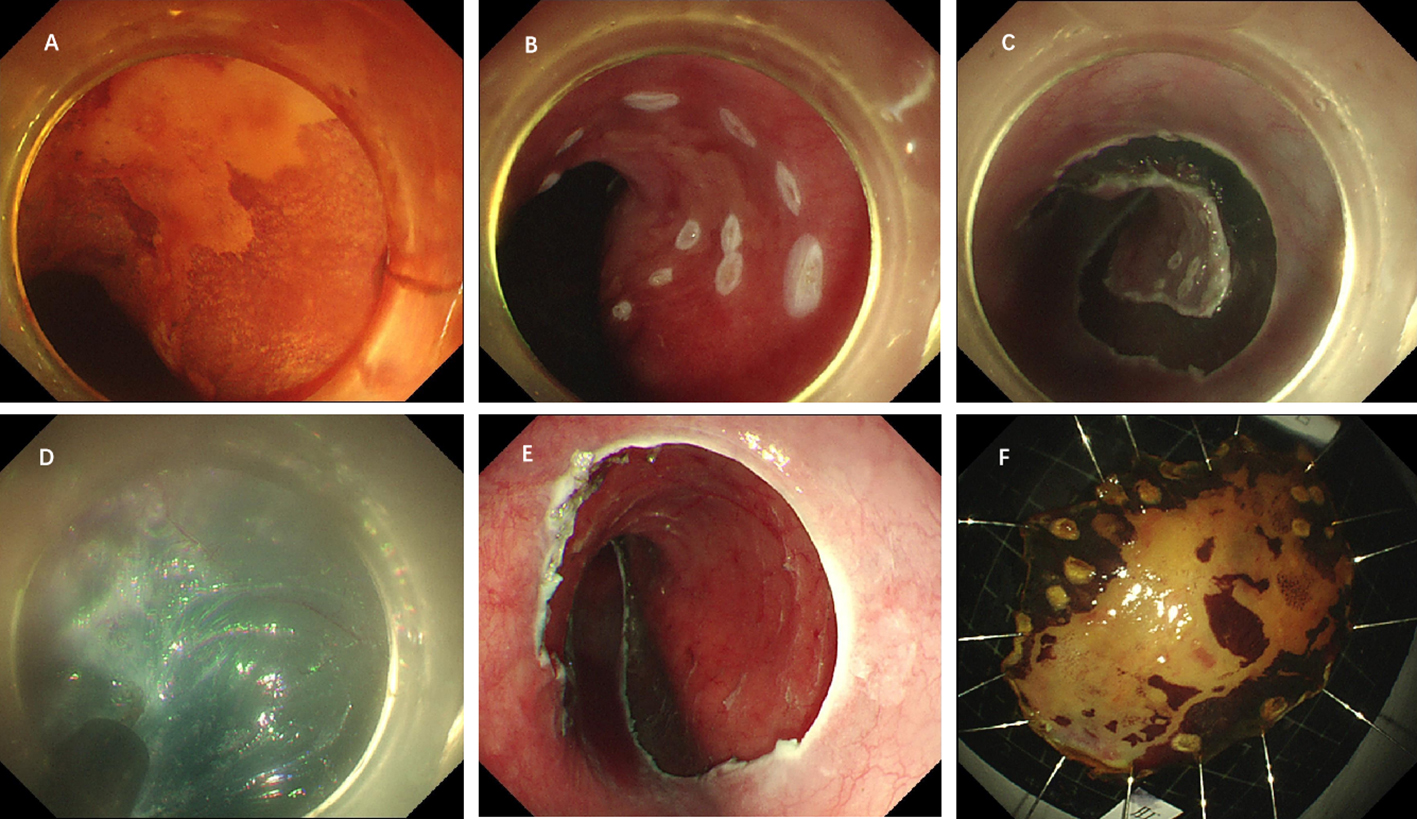
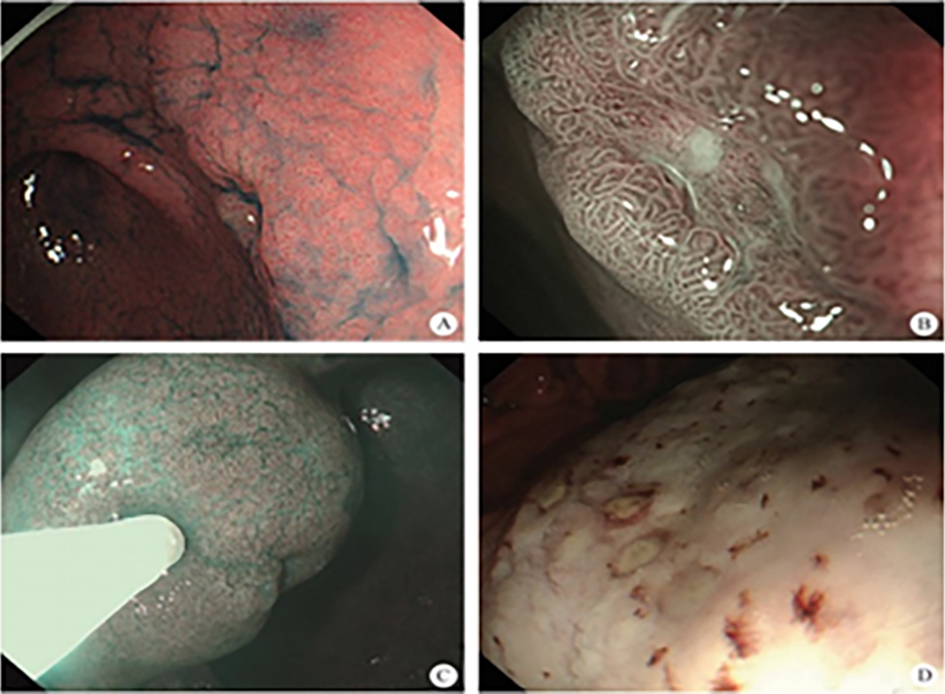
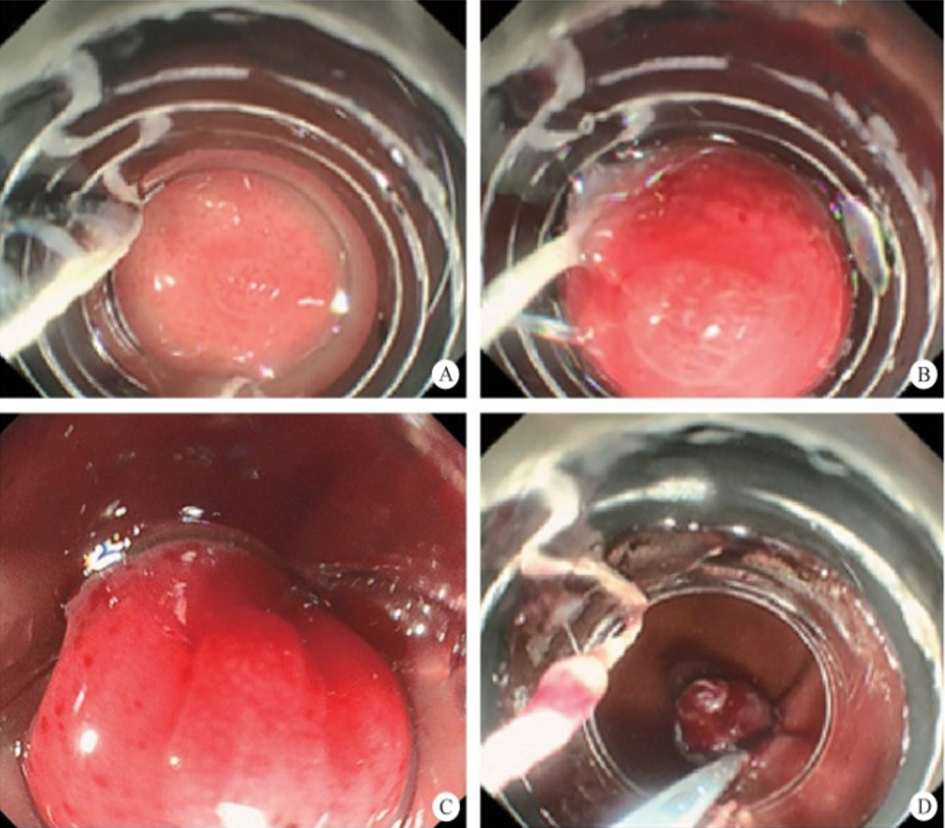
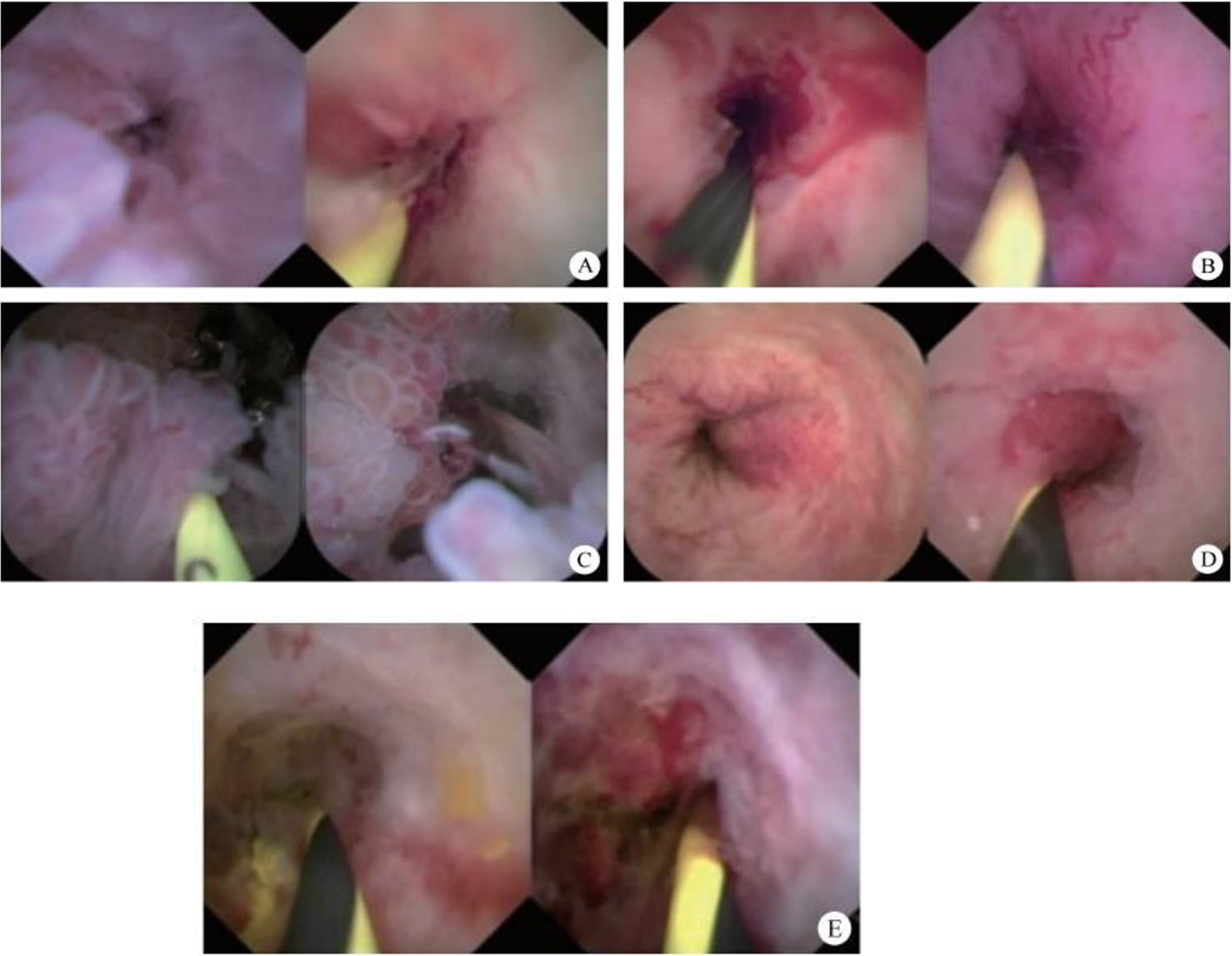
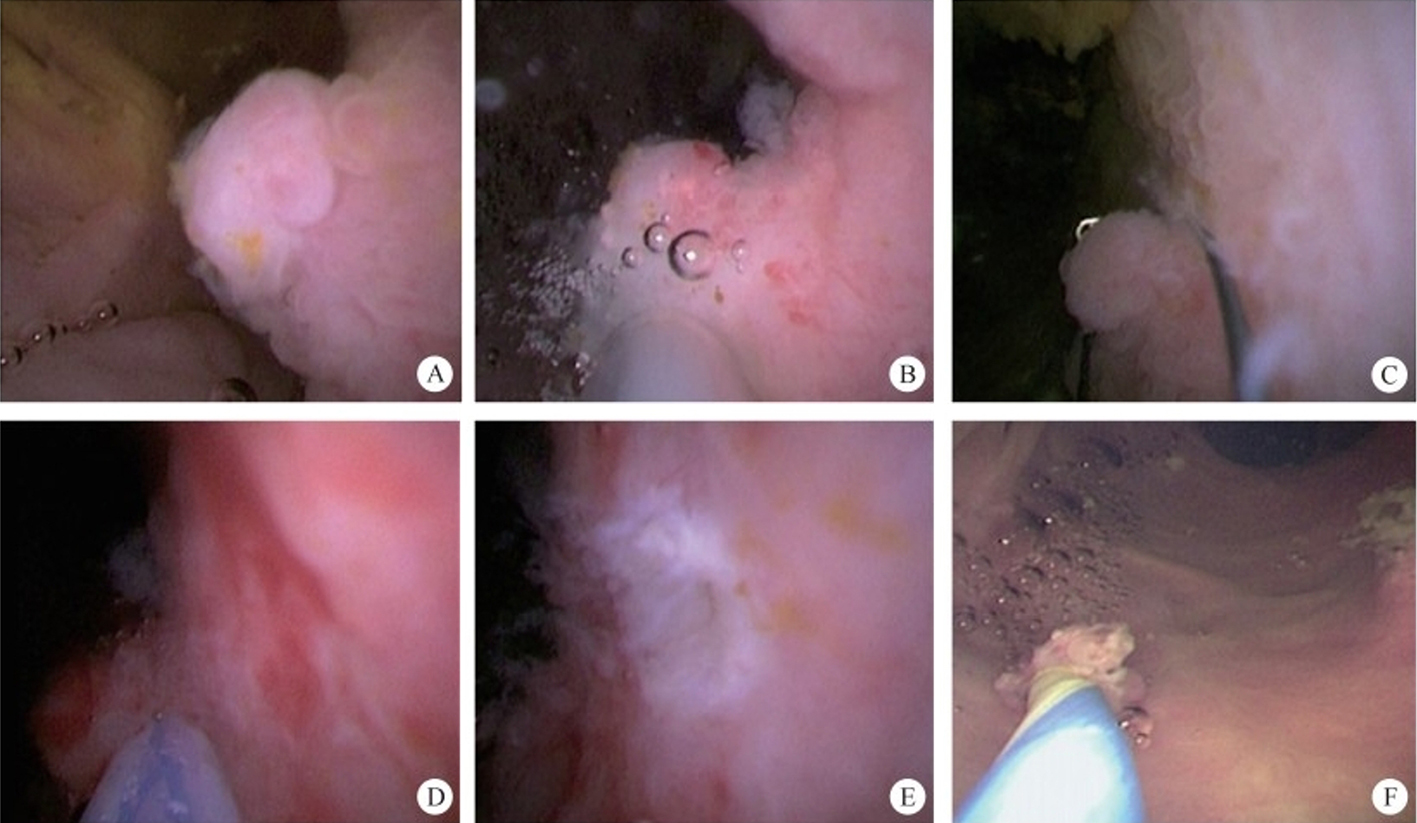
| No. | Tumor-like IBS Features |
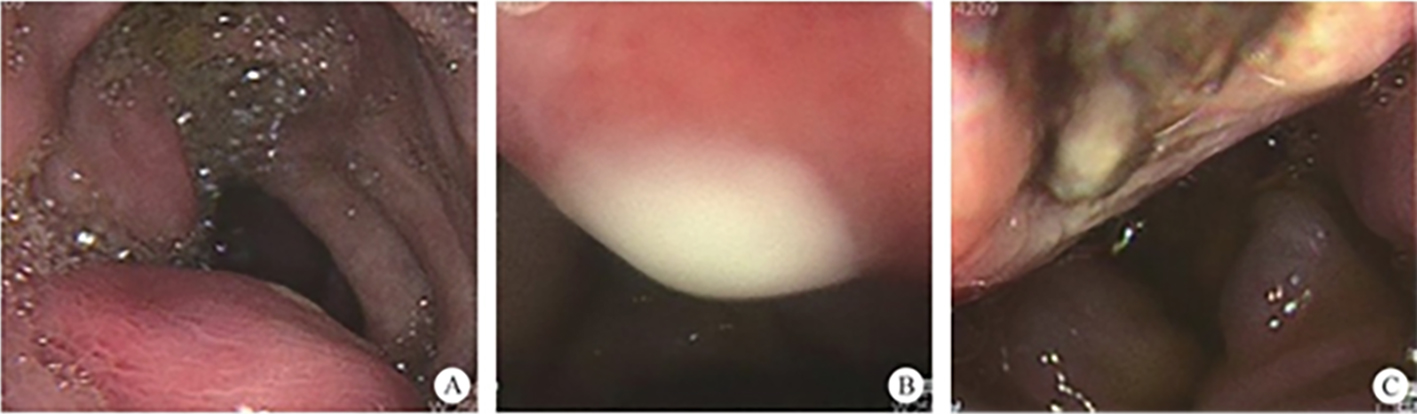
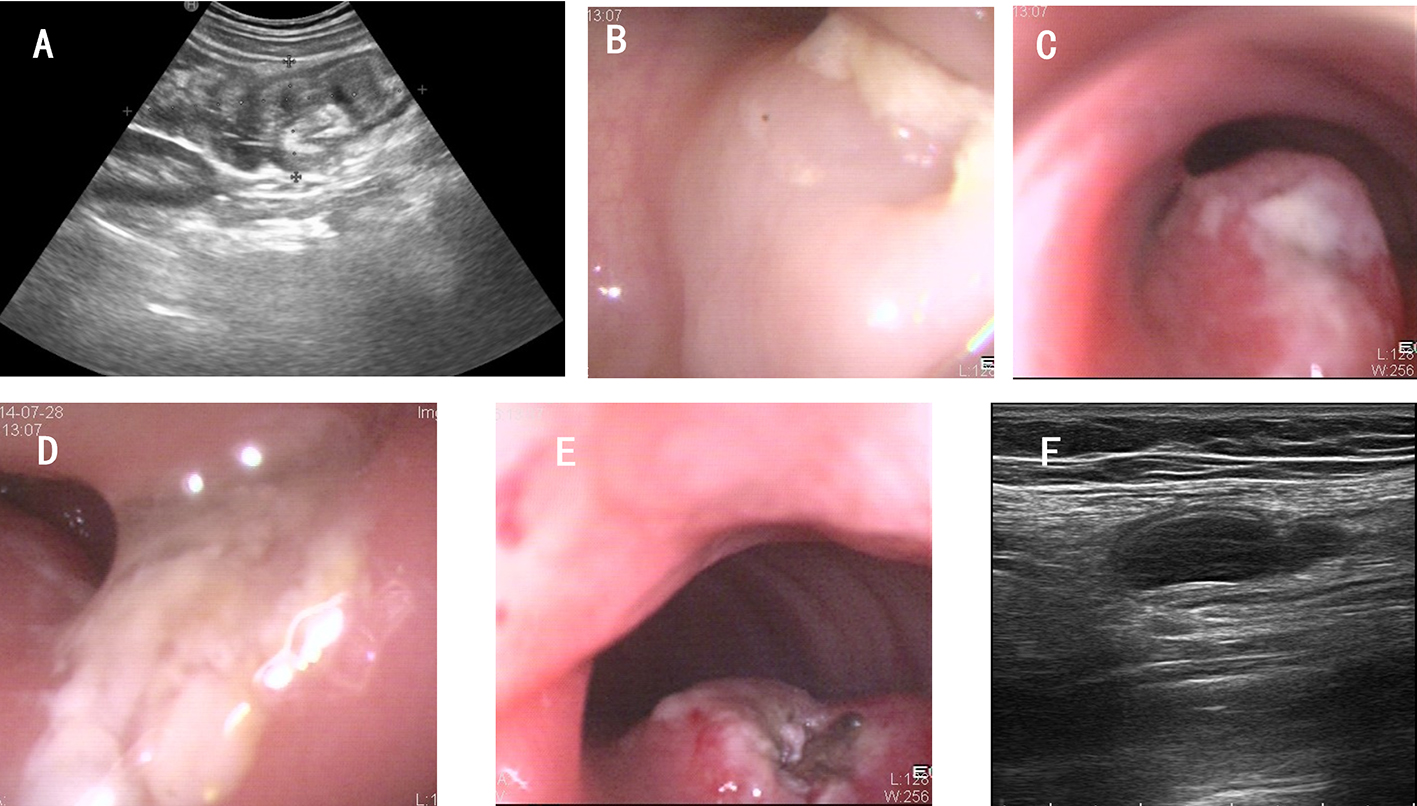
| 1 | Microvillus structures (figure 11.7A) |
| 2 | Irregular blood vessels with easy bleeding (figure 11.7B) |
| 3 | Lobular papillary structures (figure 11.7C) |
| 4 | Dam-like elevations (figure 11.7D) |
| 5 | Mucosal erosion and rough texture (figure 11.7E) |
| Diagnostic criteria | If one of the above five features is present, the lesion can be classified as a tumor-like lesion. If none of the features are present, the lesion can be classified as non-tumor-related. |
11.3 Super Minimally Invasive Drainage for Biliary Fistulae
11.4 Super Minimally Invasive Surgery for Gallbladder Stones and Cholecystitis
11.4.1 Overview
11.4.2 Gallbladder Stones: Super Minimally Invasive Stone Removal
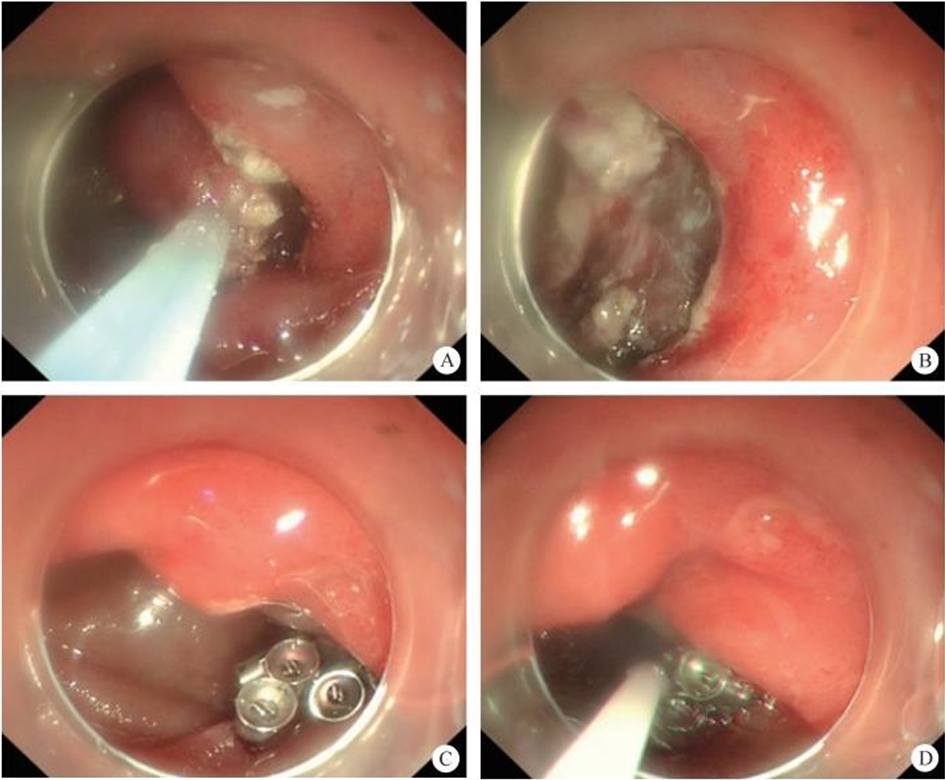
After thorough preoperative evaluation and signing of the informed consent form, the patient underwent SMIS choledochoscopy and stone extraction for gallbladder sludge-like stones (Refer to video 11.2, Gallbladder stone removal via super minimally invasive stone fragmentation and extraction at the duodenal papilla (See online resources)).
11.4.3 Percutaneous Ultrasound-Endoscopic Guided Aspiration for Acute Suppurative Cholecystitis

11.5 Endoscopic Super Minimally Invasive Resection of Biliary Polyps
Refer to video 11.3, Peroral super minimally invasive resection of biliary polyps (See online resources).
References
Chapter 12 Super Minimally Invasive Surgery for Pancreatic Diseases
12.1 Super Minimally Invasive Sclerotherapy with Polidocanol
12.1.1 Overview
12.1.2 Diagnosis
12.1.3 Indications and Contraindications for Endoscopic Polidocanol Ablation of Pancreatic Cystic Neoplasms
12.1.4 Preoperative Preparation
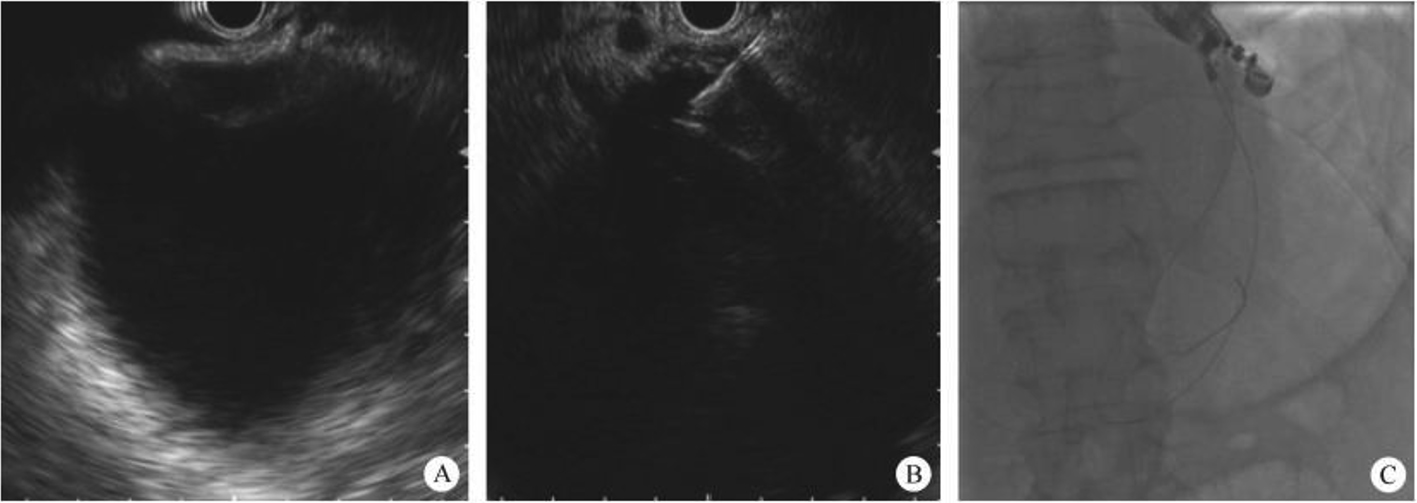
12.1.5 Surgical Procedure and Techniques (Figure
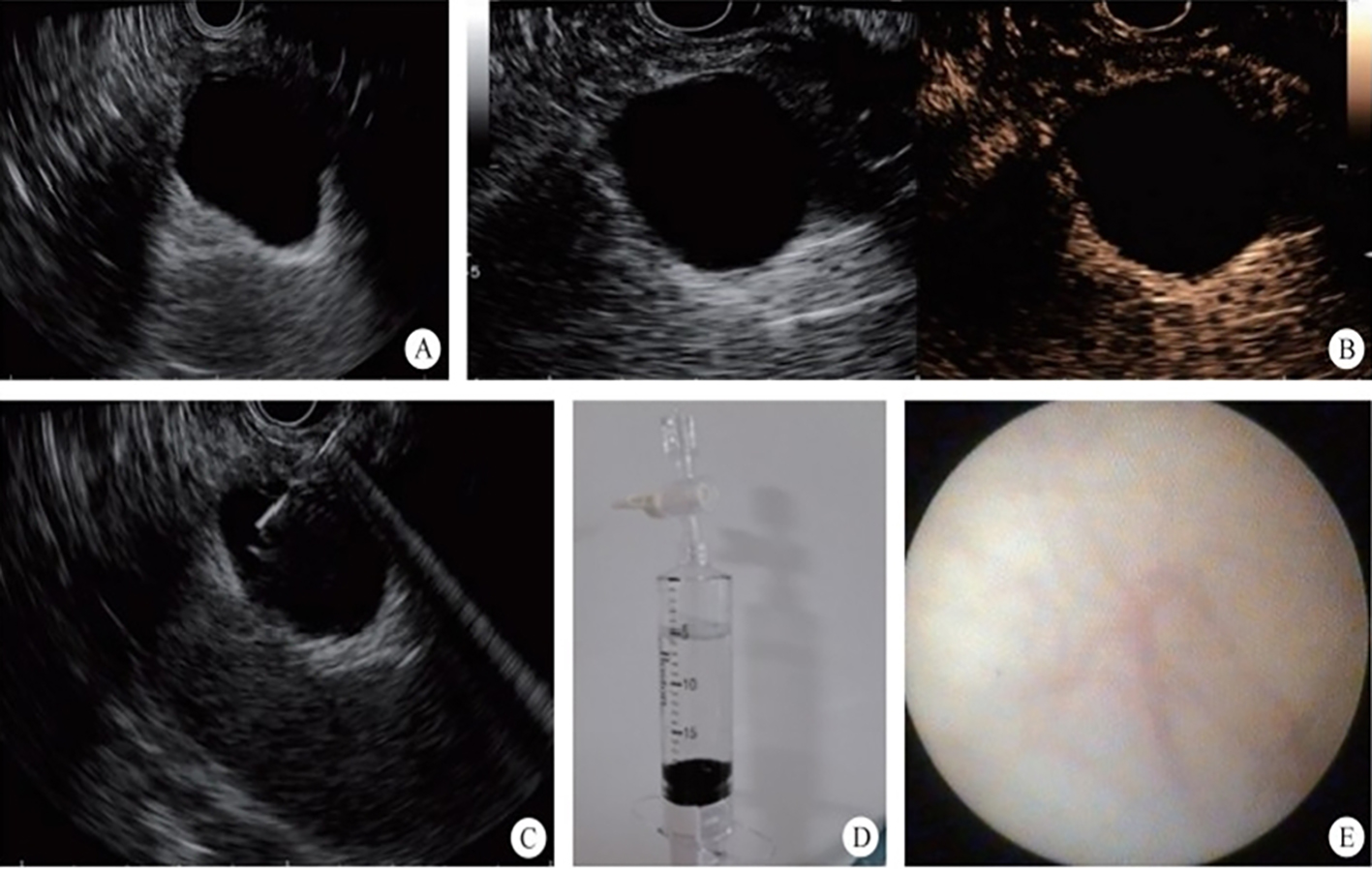
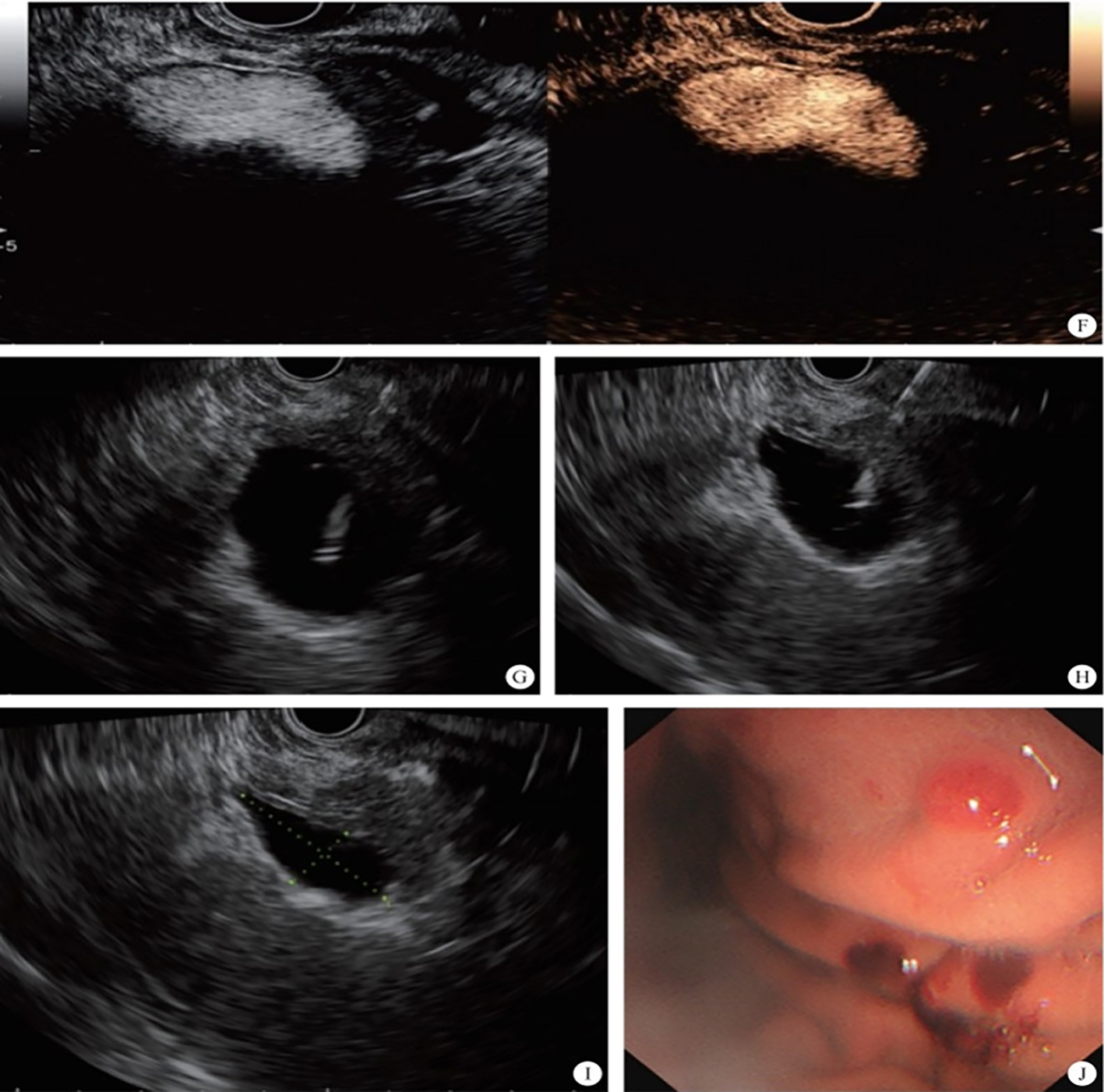
Refer to video 12.1, Super minimally invasive polidocanol ablation for pancreatic cystic tumors via a puncture channel (See online resources).
12.1.6 Postoperative Management
12.1.7 Postoperative Follow-Up
12.1.8 Hot-Spot Issues and Research Progress in the Consensus
12.2 Super Minimally Invasive Removal of Pancreatic Duct Stones
12.2.1 Overview
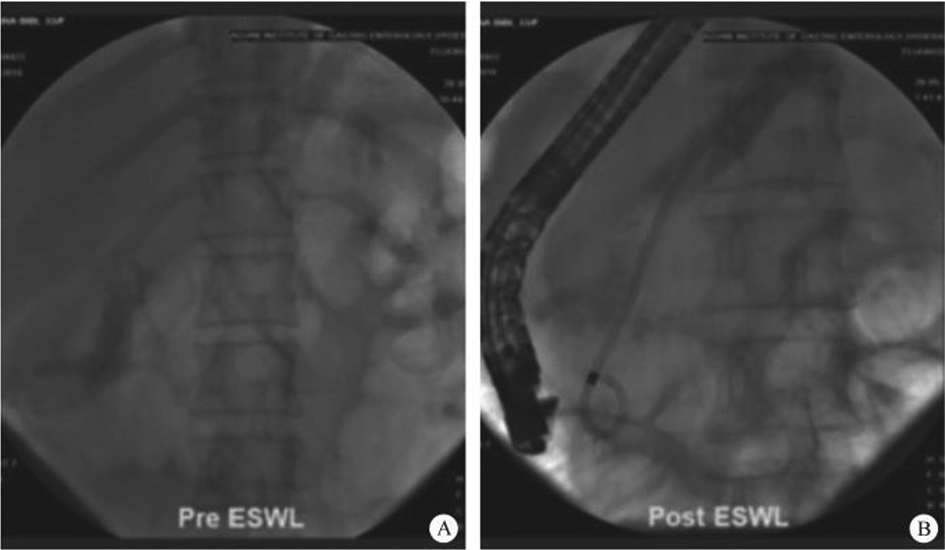
12.2.2 Endoscopic Super Minimally Invasive Removal of Pancreatic Duct Stones via the Duodenal Papilla + Extracorporeal Shockwave Lithotripsy (ESWL)
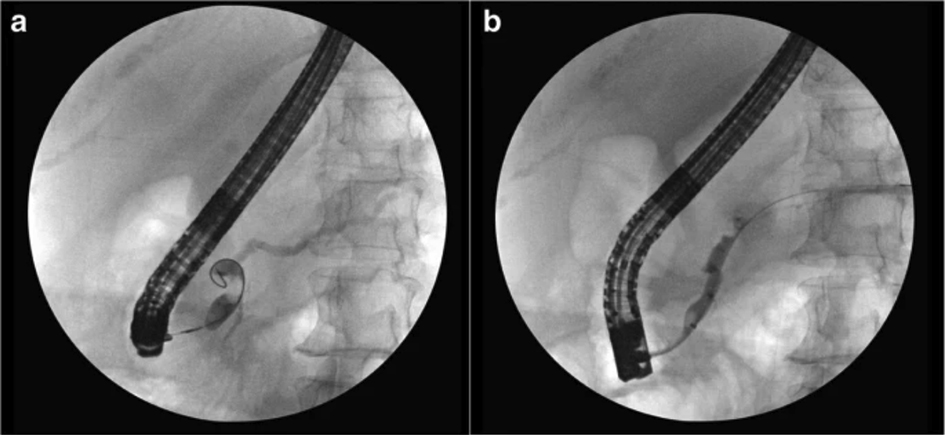
12.2.3 Pancreatic Duct Stones and Super Minimally Invasive Stone Removal via Pancreatoscopy
12.3 Pancreatic Fistula – Super Minimally Invasive Drainage
12.3.1 Overview
12.3.2 Diagnosis of Pancreatic Fistula
12.3.3 Indications and Contraindications for Endoscopic Super Minimally Invasive Drainage of Pancreatic Fistula
12.3.4 Surgical Methods and Procedures
12.3.5 Hot-Spot Issues in the Consensus
12.4 Pancreatic Walled-Off Necrosis: Super Minimally Invasive Drainage
12.4.1 Overview
12.4.2 Diagnosis of WON
12.4.3 Indications and Contraindications
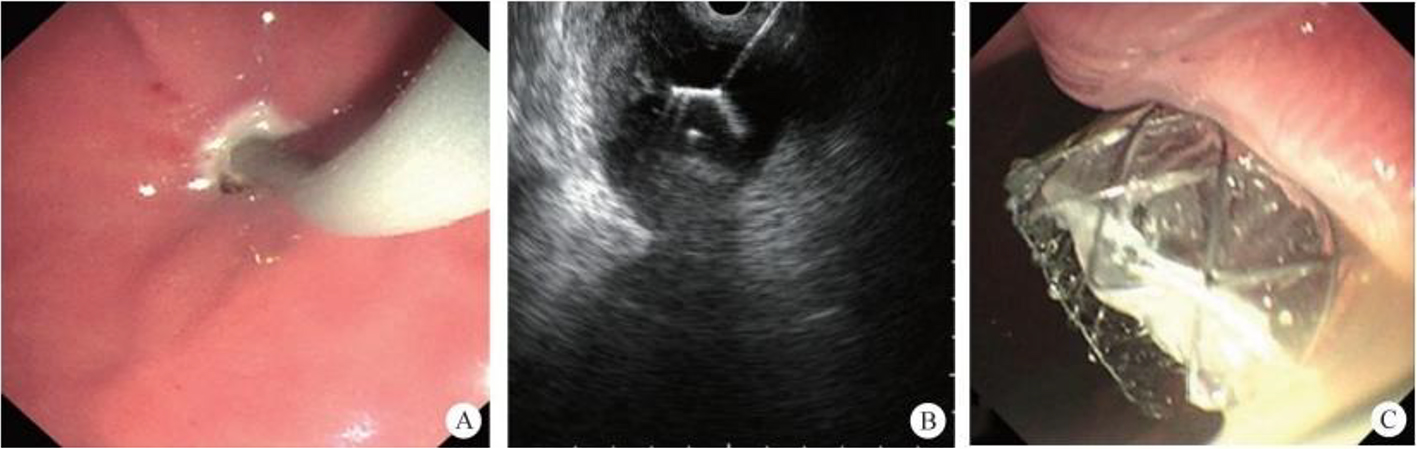
12.4.4 Surgical Procedures and Techniques
12.4.5 Postoperative Management
12.4.6 A Classic Case
Refer to video 12.2, Super minimally invasive drainage of pancreatic walled-off necrosis via a gastric puncture pathway (See online resources).
12.4.7 Hot-Spot Issues and Research Progress in the Consensus
References
Chapter 13 Super Minimally Invasive Surgery of Colorectal Diseases
13.1 Resection of Early Colorectal Cancer by Super Minimally Invasive Surgery
13.1.1 Overview
| No. | Super Minimally Invasive Surgery (SMIS) | Technical Method | Previous Nomenclature |
| 1 | Early colorectal cancer peroral super minimally invasive resection | Peranal endoscopic local resection | Endoscopic submucosal dissection (ESD) traction-assisted endoscopic submucosal dissection |
| Cap-assisted endoscopic mucosal resection endoscopic mucosal resection (EMR) | |||
| 2 | Peroral super minimally invasive resection for early colorectal cancer | Super minimally invasive full-thickness resection | Endoscopic submucosal full-thickness resection |
| 3 | Per-tunnel super minimally invasive resection for early colorectal cancer | Super minimally invasive non-full-thickness resection | Traction-assisted endoscopic full-thickness resection |
| Endoscopic tunnel technique for submucosal dissection | |||
| Traction-assisted endoscopic submucosal dissection |
13.1.2 Peroral Super Minimally Invasive Non-Full-Thickness Resection for Early Colorectal Cancer
Following thorough preoperative assessment, nutritional optimization, and signed informed consent, the patient underwent peranal super minimally invasive resection of the laterally developing sigmoid colon lesion. Refer to video 13.1, Peranal super minimally invasive full-thickness resection of laterally developing lesion in the colon (See online resources).
After comprehensive preoperative evaluation, nutritional optimization, and signing the surgical informed consent form, the patient underwent peranal super minimally invasive resection of early rectal cancer. Refer to video 13.2, Peranal super minimally invasive full-thickness resection of early rectal cancer (See online resources).
13.1.3 Peranal Super Minimally Invasive Full-Thickness Resection of Colorectal Cancer
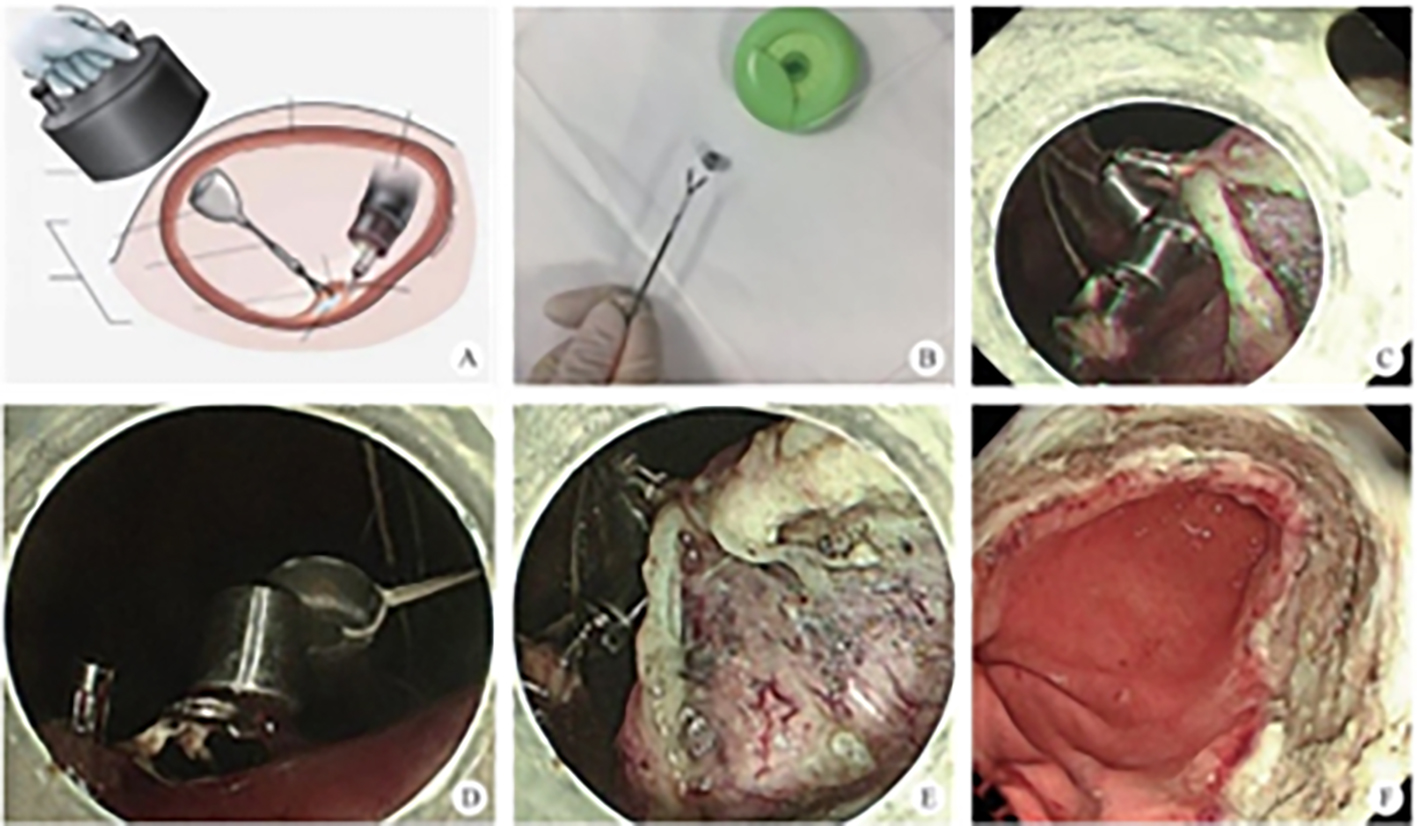
After thorough preoperative assessment, nutritional improvement, and signing of the informed consent form, the patient underwent cecal adenoma peranal super minimally invasive full-thickness resection (SMIS–EFTR). Refer to video 13.3, Peranal super minimally invasive full-thickness resection for early cecal cancer (See online resources).
After thorough preoperative assessment, nutritional improvement, and signing of the informed consent form, the patient underwent peranal super minimally invasive full-thickness resection (SMIS–EFTR) of early-stage ascending colon cancer. Refer to video 13.4, Peranal super minimally invasive full-thickness resection for early ascending colon cancer (See online resources).
After thorough preoperative evaluation, nutritional optimization, and signing the informed consent form, the patient underwent peranal super minimally invasive full-thickness resection (SMIS–EFTR) for rectal cancer after treatment (cCR). Refer to video 13.5, Rectal cancer post-chemoradiotherapy treated by peranal super minimally invasive full-thickness resection (See online resources).
13.1.4 Early Rectal Cancer: Endoscopic Submucosal Tunnel Dissection
After a thorough preoperative evaluation, nutritional status improvement, and obtaining informed consent for surgery, the patient underwent peranal super minimally invasive resection (SMIS–ESTD) for the rectal lesion. Refer to video 13.6, Super minimally invasive resection of early rectal cancer through a tunnel channel (See online resources).
13.2 Super Minimally Invasive Resection of Colorectal Subepithelial Lesions
13.2.1 Overview
| No. | Super Minimally Invasive Surgery (SMIS) | Technical Method | Previous Name |
| 1 | Peranal super minimally invasive submucosal tumor resection of colorectal epithelium | Super minimally invasive non-total layer resection | Endoscopic submucosal dissection (ESD), traction-assisted endoscopic submucosal dissection (TA-ESD) |
| 2 | Peranal super minimally invasive submucosal tumor resection of colorectal epithelium | Super minimally invasive full-thickness resection | Cap-assisted endoscopic mucosal resection (EMR), endoscopic mucosal resection (EMR), endoscopic submucosal tumor excavation, endoscopic full-thickness resection, traction-assisted endoscopic full-thickness resection |
| 3 | Peranal super minimally invasive tunnel resection of colorectal submucosal tumors | Super minimally invasive non-total layer resection | Endoscopic tunnel submucosal dissection (ETSD) |
| 4 | Peranal super minimally invasive multi-lumen channel resection of colorectal submucosal tumors | Multi-lumen channel super minimally invasive resectionTraction-assisted endoscopic submucosal dissection | Multi-endoscope combined therapy |
13.2.2 Peranal Super Minimally Invasive Resection of Colorectal Submucosal Tumors
Refer to video 13.7, Peranal super minimally invasive non-full-thickness layer resection of rectal subepithelial tumors (See online resources).
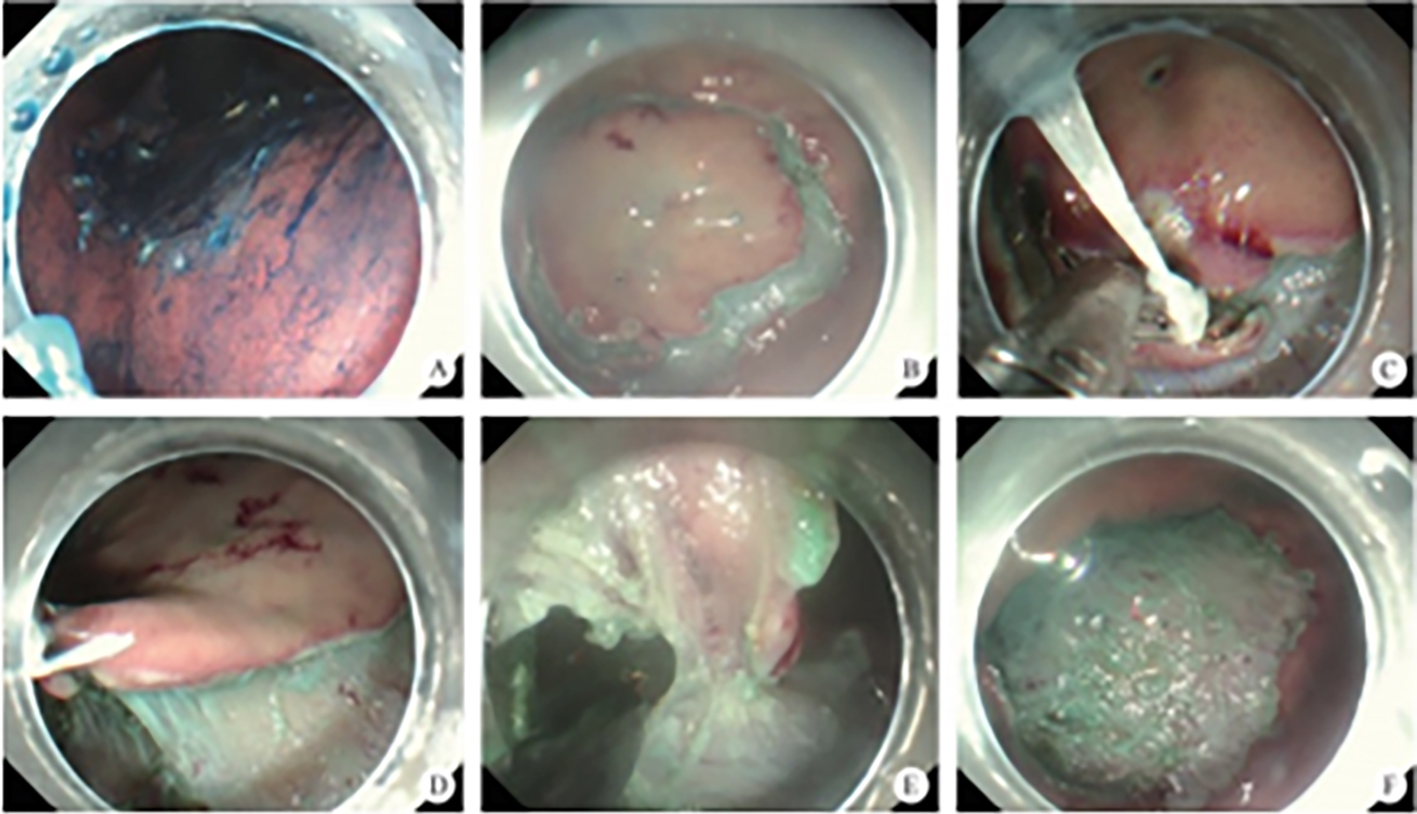
13.2.3 Neoadjuvant Therapy Followed by Peranal Super Minimally Invasive Resection of Rectal Stromal Tumors
After comprehensive preoperative evaluation, improvement of nutritional status, and obtaining informed consent for surgery, the patient underwent peranal super minimally invasive resection of rectal GIST. Refer to video 13.8, Peranal super minimally invasive full-thickness resection of a GIST in the retum (See online resources).
13.3 Super Minimally Invasive Resection of Laterally Spreading Tumors in the Colon and Rectum
13.3.1 Overview
13.3.2 Endoscopic Super Minimally Invasive Resection of Laterally Spreading Tumors (LST) in the Rectum
Refer to video 13.9, Super minimally invasive non-full-thickness resection for rectal tumors (See online resources).
13.4 Appendiceal Diseases – Super Minimally Invasive Surgery
13.4.1 Acute Appendicitis – Super Minimally Invasive Drainage via the Anus
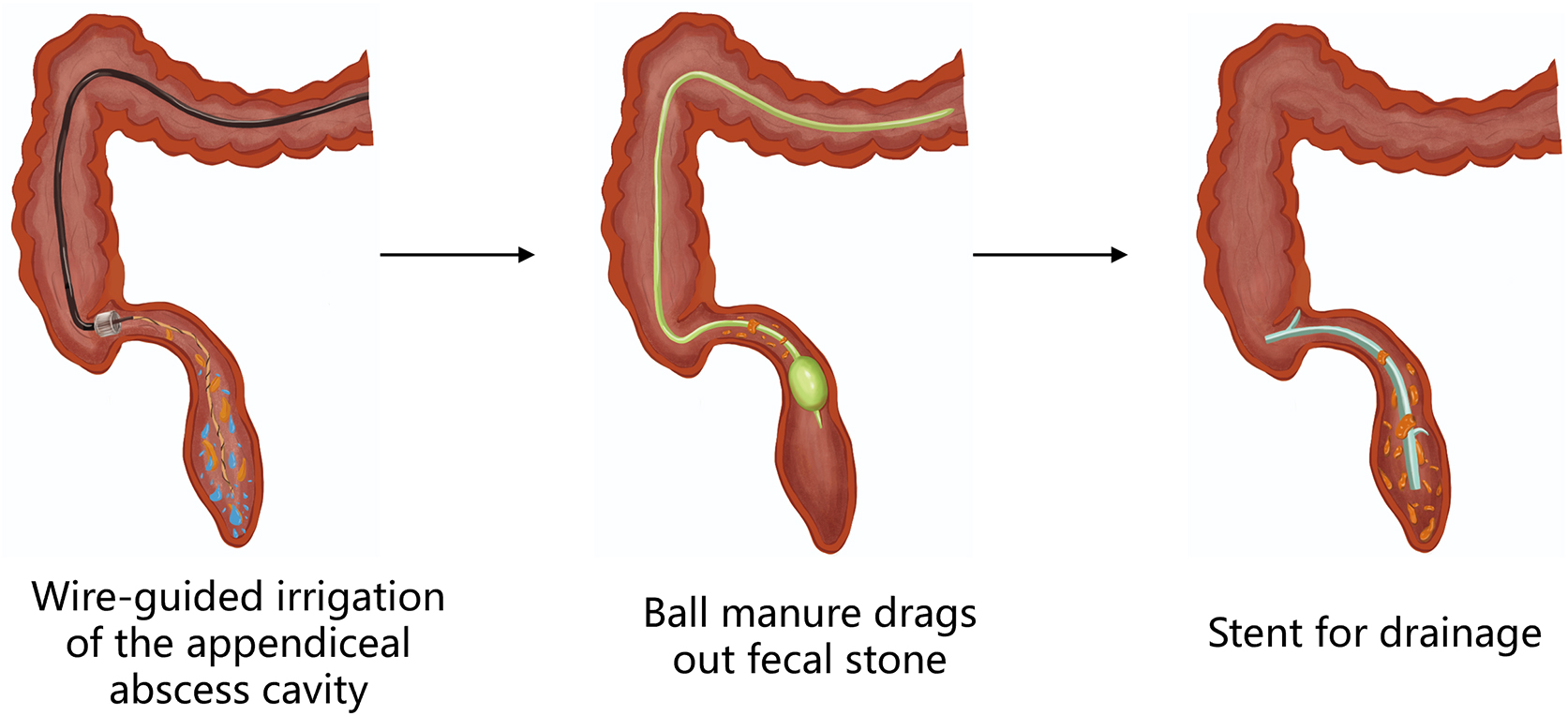
13.4.2 Super Minimally Invasive Trans-Rectal Removal of Appendicoliths using Endoscopic Retrograde Appendicitis Therapy (ERAT)
13.4.3 Periappendiceal Abscess – Super Minimally Invasive Trans-Rectal Drainage
References
Chapter 14 Super Minimally Invasive Surgery for Other Systemic Diseases
14.1 Super Minimally Invasive Weight Loss Surgery for Obesity
14.1.1 Overview
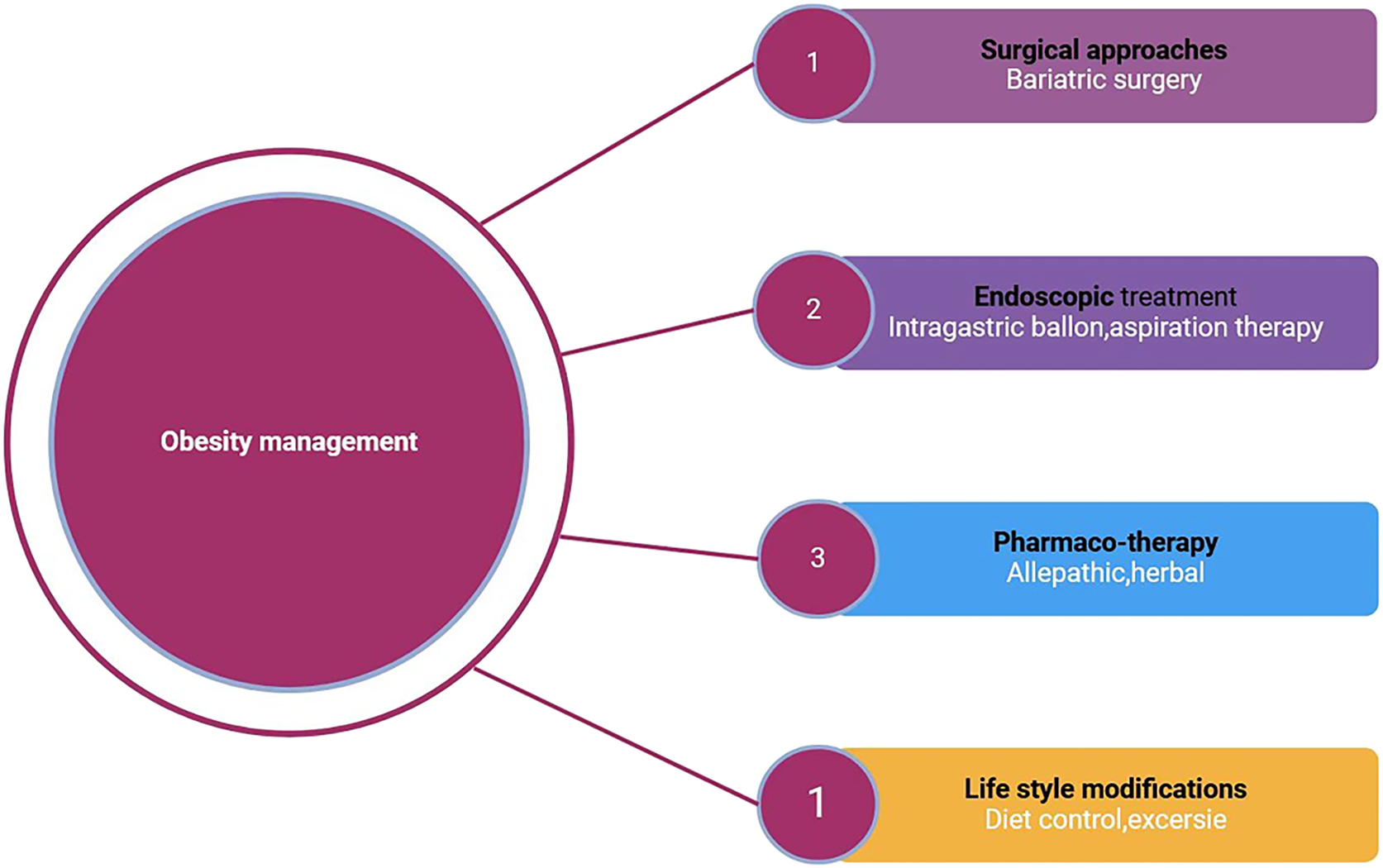
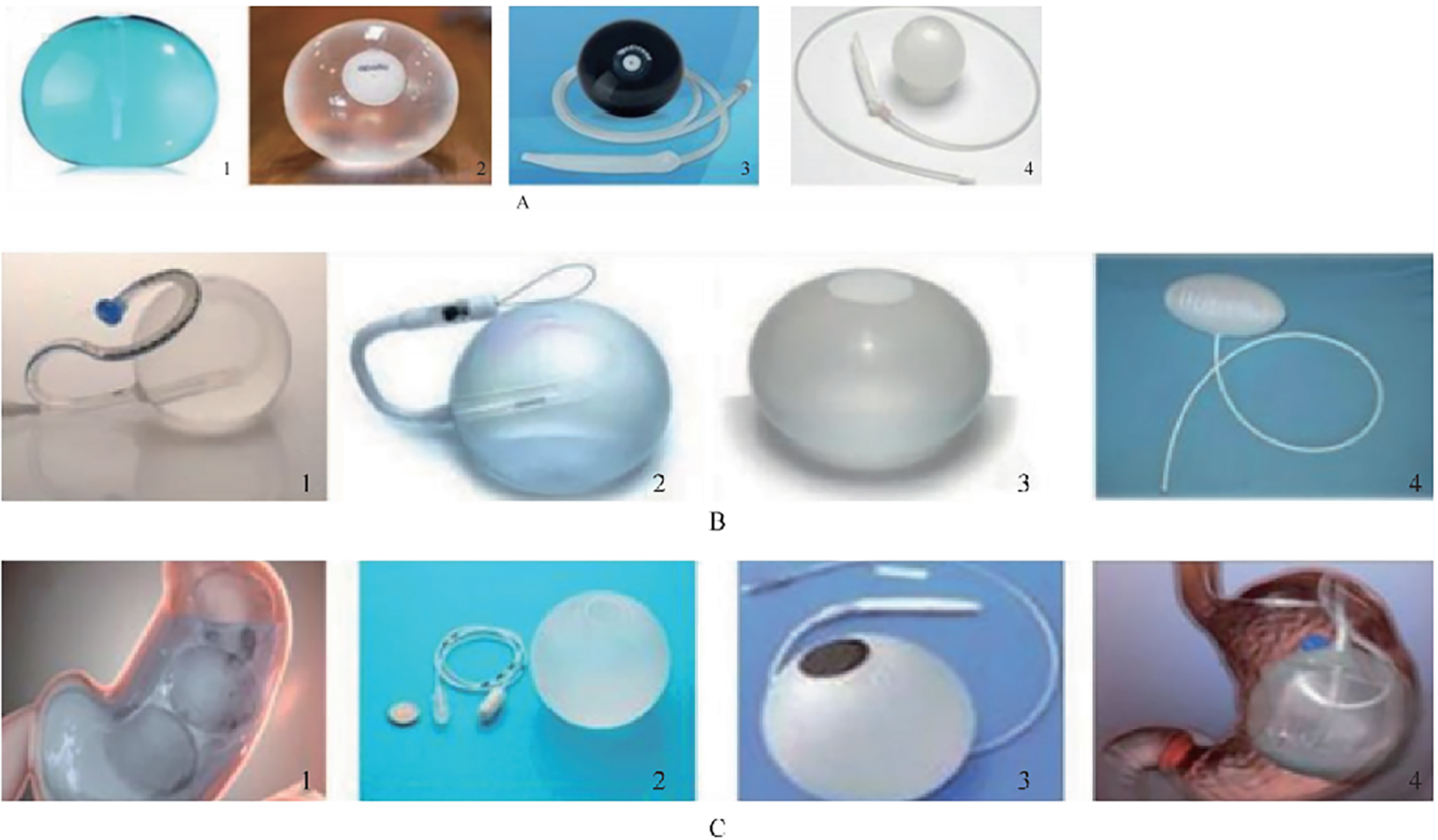
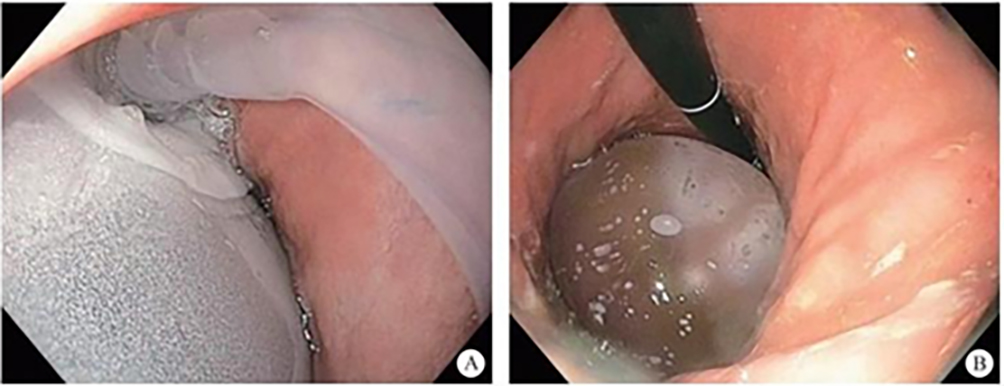
14.1.2 Intragastric Balloon Placement for Weight Loss
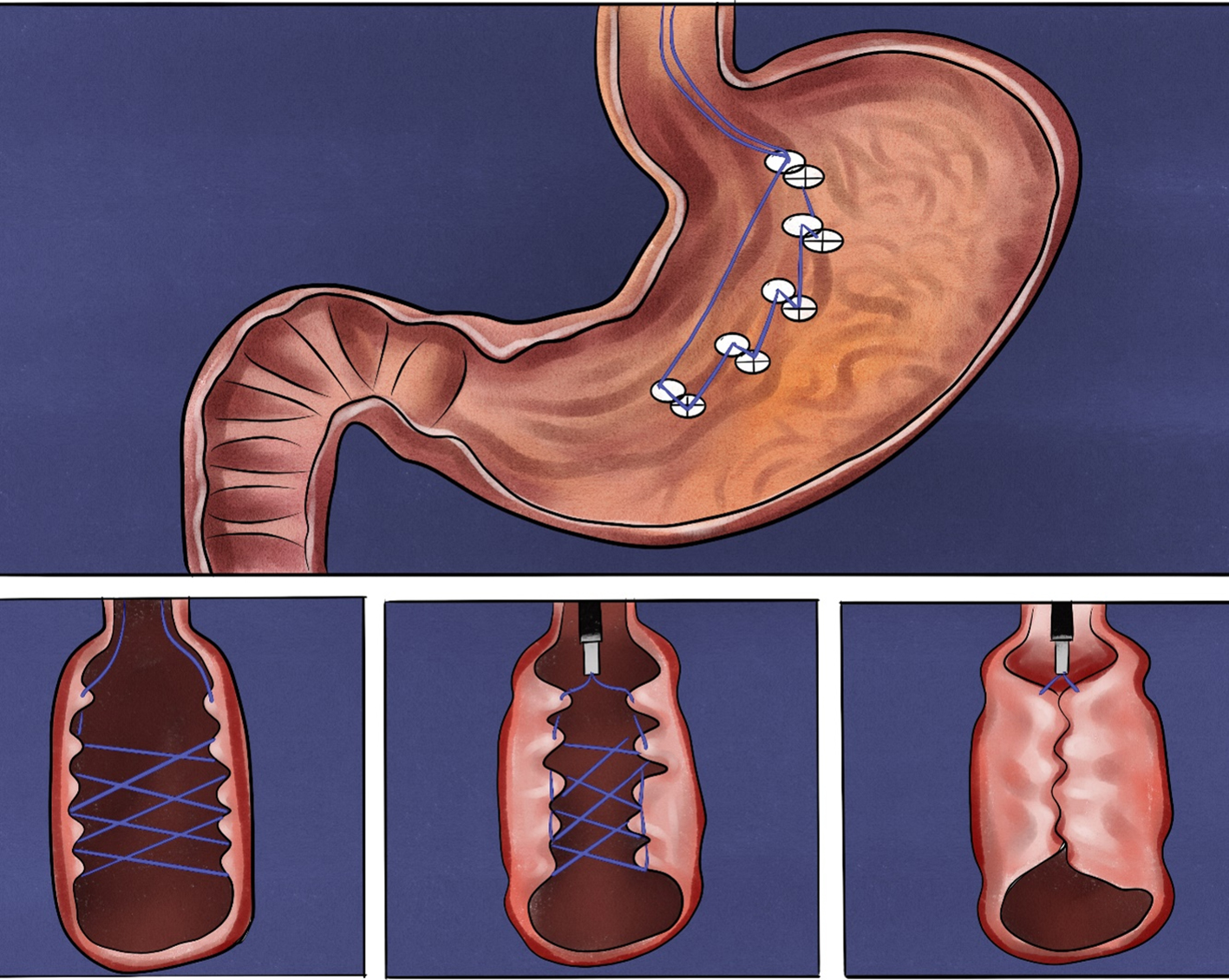
14.1.3 Endoscopic Sleeve Gastroplasty (ESG)
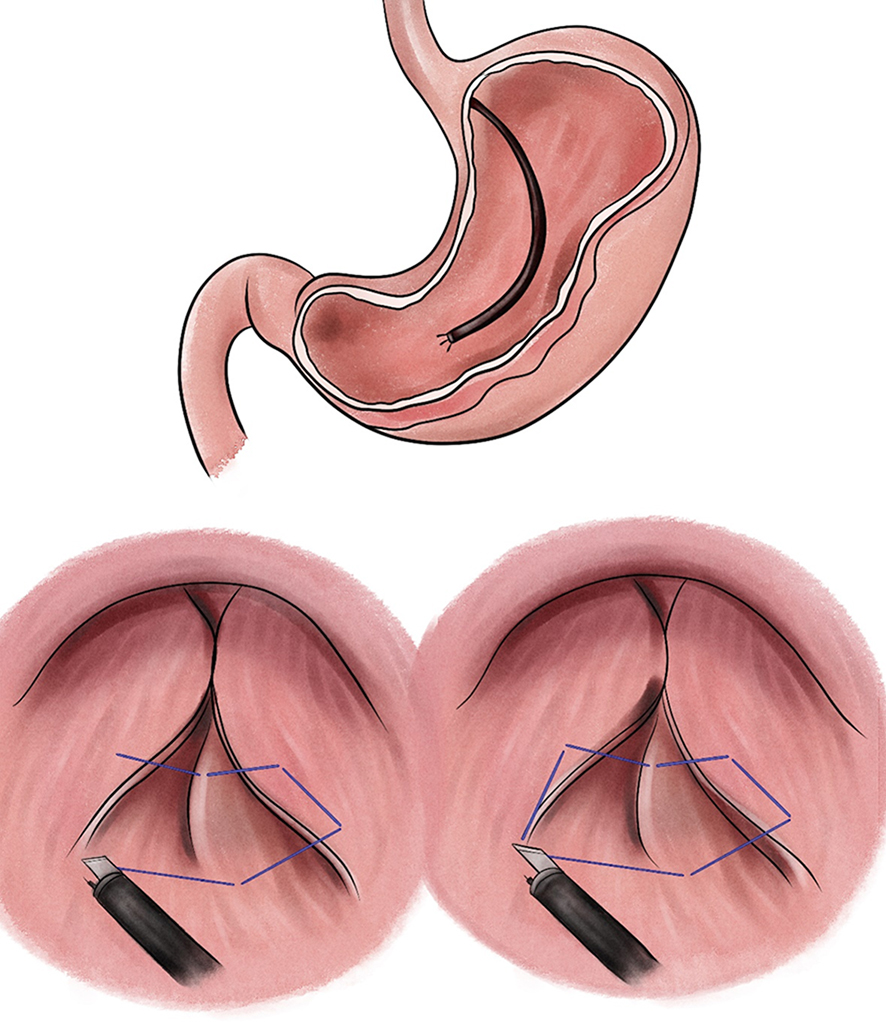
14.1.4 Endoluminal Vertical Gastroplasty (EVG)
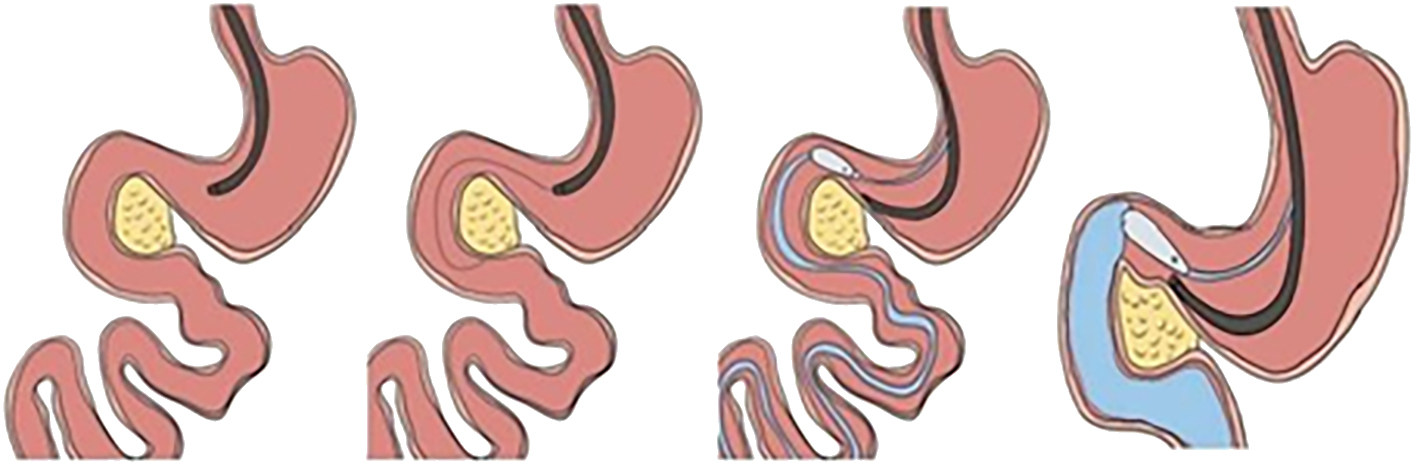
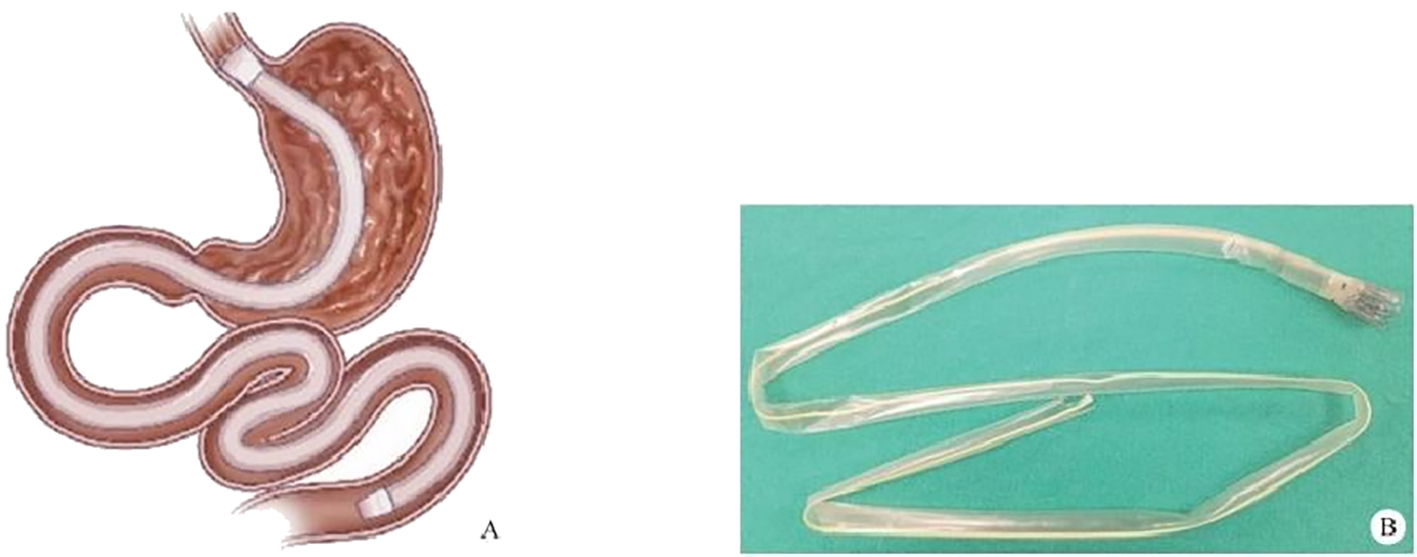
14.1.5 Endoscopic Duodenojejunal Bypass Sleeve (EDJBS)
14.1.6 Endoscopic Gastro-Duodenal-Jejunal Bypass Sleeve Surgery
14.2 Super Minimally Invasive Drainage of Mediastinal and Abdominopelvic Abscesses
14.2.1 Overview
14.2.2 Clinical Symptoms and Diagnosis
14.2.3 Indications and Contraindications of Super Minimally Invasive Drainage
14.2.4 Preoperative Preparation
14.2.5 Surgical Procedure
14.2.6 Postoperative Management
14.2.7 Hot-Spot Issues and Discussion in the Consensus
References
Appendix
| SMIS channel | Title | References |
| Natural orifice channel | (Video 2.1) A modified endoscopic resection of the entire thickness of a gastrointestinal stroma tumor: A new sealing technique based on the principles of super minimally invasive surgery(Video 2.2) Novel endoscopic papillectomy technique for reducing postoperative adverse events(Video 2.3) Successful endoscopic transgastric retrieval of a plastic stent that migrated into the abdominal cavity during pancreatic fistula drainage.(Video 2.4) Endoscopic retrieval of a migrated lumen-apposing metal stent into the abdominal cavity during transluminal drainage(Video 2.5) Incidental discovery of a pancreatic ductal adenocarcinoma during percutaneous cholangioscopy through a T-tube tract(Video 2.6) Three pancreatic duct lesions discovered at an early stage in a patient by cholangioscopy | Endoscopy 2023, 55(S 01):E561–E562.WJG 2020, 26(40):6250-6259.Endoscopy 2020, 52(8):E289–E290.AJG 2020, 115(4):504.Endoscopy, 2023, 55:E404–E405. Endoscopy, 2023, 55:E332–E333. |
| Tunnel channel | (Video 2.7) Autologous skin-grafting surgery for the prevention of esophageal stenosis after complete circular endoscopic submucosal tunnel dissection(Video 2.8) Challenging use of the digestive endoscopic tunnel technique to treat schwannoma originating in the trachea(Video 2.9) Endoscopic submucosal tunnel dissection with an elastic traction device for a circumferential superficial esophageal neoplasm(Video 2.10) Magnetic multi-directional anchoring-guided endoscopic submucosal tunnel dissection for large gastric lesions(Video 2.11) Simultaneous performance of one-tunnel per-oral endoscopic myotomy, submucosal tunnel endoscopic resection, and diverticulotomy(Video 2.12) Peroral endoscopic myotomy with simultaneous submucosal and muscle dissection for achalasia with severe interlayer adhesions(Video 2.13) Moving the knife’s tip on the thoracic aorta: high-risk submucosal tunneling endoscopic resection procedure for a puzzling submucosal tumor in the esophagus(Video 2.14) Prepyloric submucosal tunneling endoscopic resection for a case of inflammatory mass | Endoscopy 2024, 56(S 01): E290–E291.Am J Gastroenterol 2020, 115(5):650.Endoscopy 2023, 55(S 01):E388–E389.Endoscopy 2021, 53(10):E382–E383.Gastrointest Endosc 2016, 84(5):846–847.Gastrointest Endosc 2016, 83(3):651–652.Dig Endosc 2018, 30(3):397–398.Dig Endosc 2018, 30(4):546–547. |
| Puncture channel | (Video 2.15) Rendezvous-assisted endoscopic retrograde pancreatography in a patient with annular pancreas and coexisting pancreas divisum(Video 2.16) Novel treatment of pancreatic cystic neoplasms: EUS-guided radiofrequency ablation combined with lauromacrogol ablation(Video 2.17) Spyglass discovery of a mucinous cystic neoplasm by introducing an optical fiber into the cyst through a 19G needle during EUS examination | Endoscopy 2023, 55(S 01):E559–E560.Turk J Gastroenterol 2018, 29(1):101–104.Endosc Ultrasound 2019, 8(1):60–62. |
| Multi-space channel | (Video 2.18) Flexible choledochoscopy via the cystic duct combined with laparoscopic cholecystectomy for the treatment of cholelithiasis | Endoscopy 2023, 55(S 01): E659–E661. |
| No. | Chapter Section | Title | SMIS Procedure |
| 1 | Section 8.1 | (Video 8.1) Peroral super minimally invasive resection for early esophageal carcinoma | Traction-assisted endoscopic submucosal dissection |
| 2 | Section 8.1 | (Video 8.2) Early esophageal carcinoma resection by super minimally invasive surgery through a tunnel channel | Tunnel method endoscopic submucosal dissection |
| 3 | Section 8.1 | (Video 8.3) Digestive endoscopic super minimally invasive esophageal skin grafting surgery-1 | Digestive endoscopic super minimally invasive esophageal skin grafting |
| 4 | Section 8.1 | (Video 8.4) Digestive endoscopic super minimally invasive esophageal skin grafting surgery-2 | Digestive endoscopic super minimally invasive esophageal skin grafting with autologous skin graft and medicated stent placement |
| 5 | Section 8.2 | (Video 8.5) Peroral super minimally invasive resection of esophageal subepithelial lesions through a tunnel channel | Tunnel method endoscopic submucosal tumor resection |
| 6 | Section 8.3 | (Video 8.6) Super minimally invasive radiofrequency ablation of low grade intraepithelial neoplasia | Radiofrequency ablation + APC treatment |
| 7 | Section 8.4 | (Video 8.7) Super minimally invasive prevention and treatment of peroral esophageal stenosis | Gastrointestinal stricture incision + endoscopic submucosal injection |
| 8 | Section 8.5 | (Video 8.8) Super minimally invasive cardiac constriction for gastroesophageal reflux disease | Cardia tightening procedure |
| 9 | Section 8.6 | (Video 8.9) Per-tunnel super minimally invasive myotomy for esophageal Zenker’s diverticulum | Endoscopic tunnel diverticular septum division |
| 10 | Section 8.6 | (Video 8.10) Per-tunnel super minimally invasive myotomy for lower esophageal diverticulum | Endoscopic tunnel diverticular septum division |
| 11 | Section 8.7 | (Video 8.11) Per-tunnel super minimally myotomy for achalasia-1 | Ac-iia type, peroral endoscopic myotomy |
| 12 | Section 8.7 | (Video 8.12) Per-tunnel super minimally myotomy for achalasia-2 | Post-Heller procedure, peroral endoscopic myotomy |
| 13 | Section 9.1 | (Video 9.1) Peroral super minimally invasive non-full-thickness resection for early cancer at the gastric cardia and fundus | Endoscopic submucosal dissection |
| 14 | Section 9.1 | (Video 9.2) Peroral super minimally invasive non-full-thickness resection for early cancer of the gastric body | Endoscopic submucosal dissection |
| 15 | Section 9.1 | (Video 9.3) Super minimally invasive non-full-thickness resection for early cancer of the gastric antrum | Endoscopic submucosal dissection |
| 16 | Section 9.1 | (Video 9.4) Super minimally invasive non-full-thickness resection for early gastric angular cancer | Endoscopic submucosal dissection |
| 17 | Section 9.1 | (Video 9.5) Super minimally invasive non-full-thickness resection for early cancer of the gastric antrum | Traction-assisted endoscopic submucosal dissection |
| 18 | Section 9.1 | (Video 9.6) Super minimally invasive full-thickness resection for early gastric cancer of the gastric body | Endoscopic full-thickness resection |
| 19 | Section 9.2 | (Video 9.7) Super minimally invasive radiofrequency ablation for gastric low-grade intraepithelial neoplasia | Endoscopic radiofrequency ablation |
| 20 | Section 9.3 | (Video 9.8) Super minimally invasive resection of a stromal tumor of the gastric fundus | Endoscopic submucosal excavation |
| 21 | Section 9.3 | (Video 9.9) Super minimally invasive peroral resection of subepithelial tumor of the cardia | Endoscopic submucosal excavation |
| 22 | Section 9.3 | (Video 9.10) Peroral super minimally invasive full-thickness resection of a subepithelial tumor in the gastric body | Endoscopic full-thickness resection + endoscopic suturing + assisted traction |
| 23 | Section 9.3 | (Video 9.11) Peroral super minimally invasive full-thickness resection of a tumor in the lesser sac of the gastric fundus | Endoscopic full-thickness resection + endoscopic suturing |
| 24 | Section 9.3 | (Video 9.12) Peroral super minimally invasive non-full-thickness resection of multiple gastric neuroendocrine tumors | Band ligation-assisted snare resection |
| 25 | Section 9.4 | (Video 9.13) Super minimally invasive peroral endoscopic myotomy for gastroparesis | Peroral pyloric sphincter myotomy |
| 26 | Section 10.1 | (Video 10.1) Peroral super minimally invasive non-full-thickness resection of duodenal LST | Endoscopic submucosal dissection + assisted traction |
| 27 | Section 10.2 | (Video 10.2) Peroral super minimally invasive resection of a duodenal ampullary adenoma | Snare resection + biliopancreatic duct stenting |
| 28 | Section 10.3 | (Video 10.3) Peroral super minimally invasive resection of a subepithelial tumor in the descending duodenum | Snare resection |
| 29 | Section 10.3 | (Video 10.4) Peroral super minimally invasive resection of a subepithelial tumor in the descending duodenum | Endoscopic submucosal dissection + endoscopic closure |
| 30 | Section 10.4 | (Video 10.5) Peroral super minimally invasive non-full-thickness resection of duodenal adenomas-1 | Snare resection |
| 31 | Section 10.4 | (Video 10.6) Peroral super minimally invasive non-full-thickness resection of duodenal polyps-2 | Nylon-loop-ligation-assisted resection |
| 32 | Section 11.1 | (Video 11.1) Super minimally invasive bile duct stone extraction via duodenal papillary bile duct endoscopy | Direct cholangioscopic super minimally invasive stone removal |
| 33 | Section 11.1 | 11.1 Super minimally invasive bile duct stone extraction via duodenal papillary bile duct endoscopy | Direct cholangioscopic super minimally invasive removal |
| 34 | Section 11.4 | (Video 11.2) Gallbladder stone removal via super minimally invasive stone fragmentation and extraction at the duodenal papilla | Direct cholangioscopic super minimally invasive irrigation and suction |
| 35 | Section 11.5 | (Video 11.3) Peroral super minimally invasive resection of biliary polyps | Direct cholangioscopic super minimally invasive resection |
| 36 | Section 12.1 | (Video 12.1) Super minimally invasive polidocanol ablation for pancreatic cystic tumors via a puncture channel | Super minimally invasive endoscopic lauromacrogol ablation |
| 37 | Section 12.4 | (Video 12.2) Super minimally invasive drainage of pancreatic walled-off necrosis via a gastric puncture pathway | Super minimally invasive drainage + direct visualization debridement |
| 38 | Section 13.1 | (Video 13.1) Peranal super minimally invasive full-thickness resection of laterally developing lesion in the colon | Traction-assisted endoscopic submucosal dissection + clip closure method |
| 39 | Section 13.1 | (Video 13.2) Peranal super minimally invasive full-thickness resection of early rectal cancer | Traction-assisted endoscopic submucosal dissection |
| 40 | Section 13.1 | 13.3 Peranal super minimally invasive full-thickness resection for early cecal cancer | Endoscopic submucosal full-thickness resection + assisted traction |
| 41 | Section 13.1 | (Video 13.4) Peranal super minimally invasive full-thickness resection for early ascending colon cancer | Endoscopic submucosal full-thickness resection + assisted traction |
| 42 | Section 13.1 | (Video 13.5) Rectal cancer post-chemoradiotherapy treated by peranal super minimally invasive full-thickness resection | Endoscopic submucosal full-thickness resection + assisted traction |
| 43 | Section 13.1 | (Video 13.6) Super minimally invasive resection of early rectal cancer through a tunnel channel | Endoscopic submucosal tunnel dissection |
| 44 | Section 13.2 | (Video 13.7) Peranal super minimally invasive non-full-thickness resection of rectal subepithelial tumors | Band-ligation-assisted endoscopic mucosal resection |
| 45 | Section 13.2 | (Video 13.8) Peranal super minimally invasive full-thickness resection of a lesion developing laterally in the colon | Endoscopic submucosal full-thickness resection |
| 46 | Section 13.3 | (Video 13.9) Super minimally invasive non-full-thickness resection for rectal tumor. | Pre-cutting endoscopic mucosal resection |
 复制
复制
 笔记
笔记

 高亮
高亮
 搜索
搜索

 我
2025-08-26 14:49
我
2025-08-26 14:49
 目录
笔记
搜索
目录
笔记
搜索
 笔记
笔记
 高亮
高亮




